Dell'Anna Giuseppe, Fasulo Ernesto, Cecinato Paolo, Barbara Giovanni, Barchi Alberto, Viale Edi, Esposito Dario, Grillo Simone, Sassatelli Romano, Malesci Alberto, Massironi Sara, Annese Vito, Fuccio Lorenzo, Facciorusso Antonio, Donatelli Gianfranco, Danese Silvio, Azzolini Francesco
Gastroenterology and Gastrointestinal Endoscopy, IRCCS San Raffaele Hospital, 20132 Milan, Italy.
Gastroenterology and Gastrointestinal Endoscopy, IRCCS Policlinico San Donato, 20097 San Donato Milanese, Italy.
Cancers (Basel). 2025 Apr 6;17(7):1242. doi: 10.3390/cancers17071242.
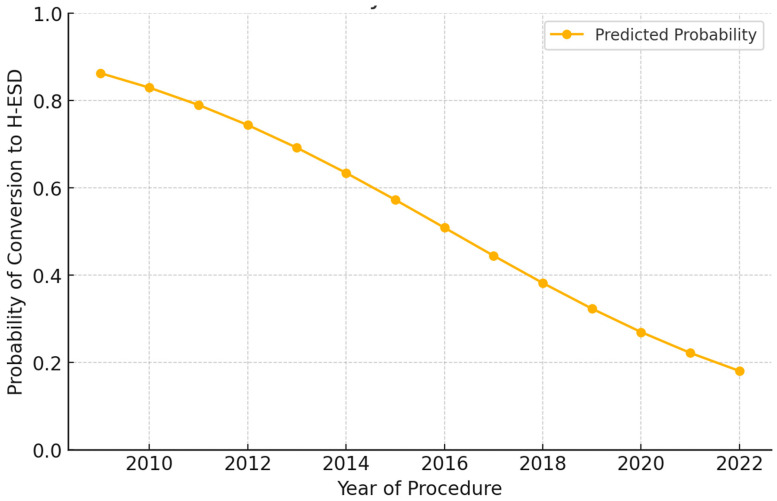
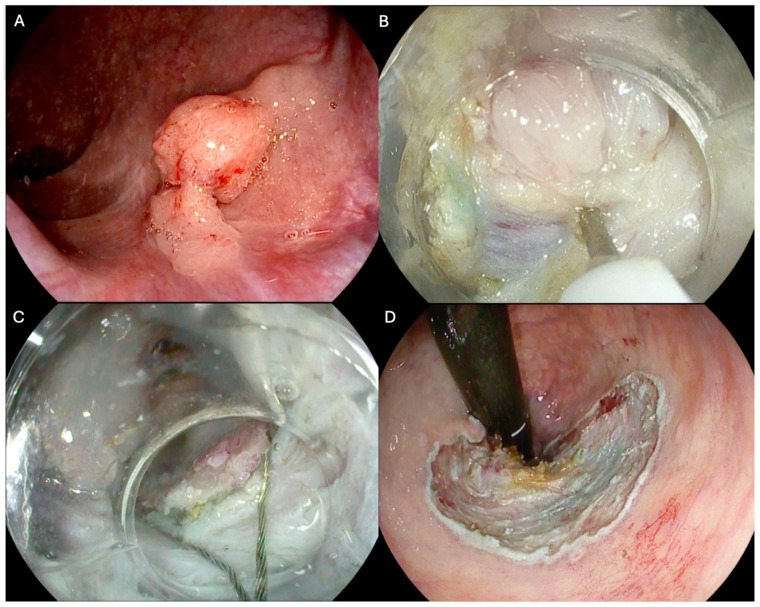
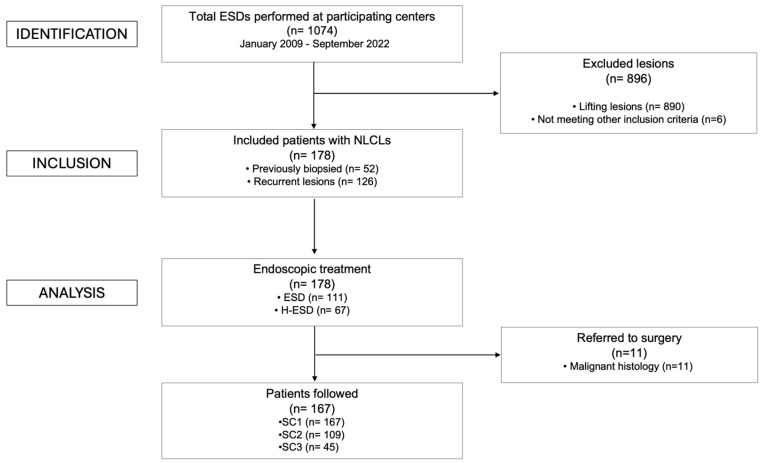
: The management of non-lifting colorectal lesions (NLCLs), often resulting from previous unsuccessful treatments or biopsies, remains challenging due to submucosal fibrosis that prevents adequate lifting. Endoscopic submucosal dissection (ESD) is a viable option for achieving complete resection in such cases. However, when standard ESD is not feasible, conversion to hybrid ESD (H-ESD) has been proposed as a rescue strategy. This study aimed to assess ESD's feasibility, effectiveness, and safety for NLCLs, including cases requiring conversion to H-ESD, when performed by experienced endoscopists in tertiary referral centers. : In this multicenter retrospective study, data from patients with NLCLs treated by ESD/H-ESD between January 2009 and September 2022 were analyzed. The primary endpoint was the recurrence rate (RR). Secondary endpoints included the adverse event (AE) rate, technical success (TS) rate (en bloc resection regardless of technique), complete resection (CR), curative resection (cR) rates, and surgical intervention rate. Predictors of ESD technical success were identified. : In total, 178 patients with NLCLs were included (52 previously biopsied, 126 recurrent after previous resection). ESD was used in 111 (62.4%) and H-ESD in 67 (37.6%) cases. During a median follow-up of 373 days (IQR 540), the overall RR was 3.6%. The overall AE rate was 13.4%, and perforation was the most frequent (8.4%). All AEs were successfully managed endoscopically. The TS rate was 71.9%, significantly higher in previously biopsied lesions compared to recurrent ones (78.8% vs. 55.6%, = 0.04). On multivariate analysis, rectal location ( < 0.001), F1 fibrosis ( = 0.026), and previously biopsied lesions ( = 0.006) predicted ESD TS without the need for conversion to H-ESD. : ESD/H-ESD is feasible and safe for NLCLs when performed by experienced operators, with low RR amenable to endoscopic treatment. Previously biopsied lesions, rectal location, and low fibrosis predict ESD TS.
非抬举性大肠病变(NLCLs)的管理常常因先前治疗或活检失败导致黏膜下纤维化而阻碍充分抬举,因而颇具挑战性。内镜黏膜下剥离术(ESD)是此类病例实现完整切除的可行选择。然而,当标准ESD不可行时,已提出转换为混合ESD(H-ESD)作为补救策略。本研究旨在评估由三级转诊中心经验丰富的内镜医师进行ESD时,其对NLCLs的可行性、有效性和安全性,包括需要转换为H-ESD的病例。
在这项多中心回顾性研究中,分析了2009年1月至2022年9月期间接受ESD/H-ESD治疗的NLCLs患者的数据。主要终点是复发率(RR)。次要终点包括不良事件(AE)率、技术成功率(TS)(无论采用何种技术的整块切除)、完整切除(CR)、根治性切除(cR)率以及手术干预率。确定了ESD技术成功的预测因素。
总共纳入了178例NLCLs患者(52例曾接受活检,126例先前切除后复发)。111例(62.4%)采用ESD,67例(37.6%)采用H-ESD。在中位随访373天(IQR 540)期间,总体RR为3.6%。总体AE率为13.4%,穿孔最为常见(8.4%)。所有AE均通过内镜成功处理。TS率为71.9%,先前活检的病变显著高于复发病变(78.8%对55.6%,P = 0.04)。多因素分析显示,直肠位置(P < 0.001)、F1纤维化(P = 0.026)和先前活检的病变(P = 0.006)预测ESD技术成功且无需转换为H-ESD。
当由经验丰富的操作者进行时,ESD/H-ESD对NLCLs是可行且安全的,RR低且适合内镜治疗。先前活检的病变、直肠位置和低纤维化预测ESD技术成功。