Dolovac Ryan Beerling, King James, Ovenden Christopher, Kam Jeremy, Wang Yi Yuen, Goldschlager Tony, Castle-Kirszbaum Mendel
School of Medicine, University of Western Australia, Perth, Australia.
Department of Neurosurgery, Royal Melbourne Hospital, Melbourne, Australia.
Pituitary. 2025 Apr 14;28(3):49. doi: 10.1007/s11102-025-01521-4.
The optimal surgical technique for managing Rathke's Cleft Cyst (RCC) remains unclear. Leaving the sellar defect open (marsupialisation) after transsphenoidal surgery facilitates ongoing drainage of cyst contents, but cannot be performed in the setting of an intraoperative cerebrospinal fluid (CSF) leak. The effects of intraoperative CSF leaks and sellar floor reconstruction on RCC recurrence require further investigation.
A systematic literature search was conducted for studies reporting RCC recurrence following transsphenoidal surgery, with data on intraoperative CSF leak rates and skull base reconstruction. Studies were classified based on surgical technique: cyst wall resection vs. fenestration, and open (no reconstruction) vs. closed (reconstructed) sellar floor.
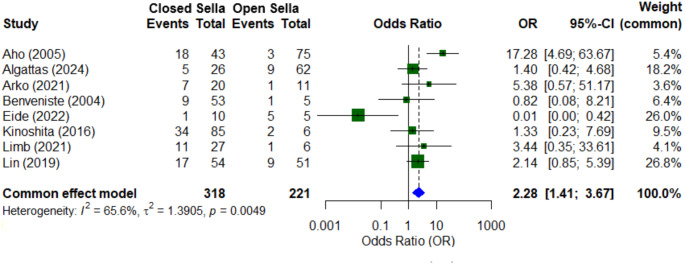
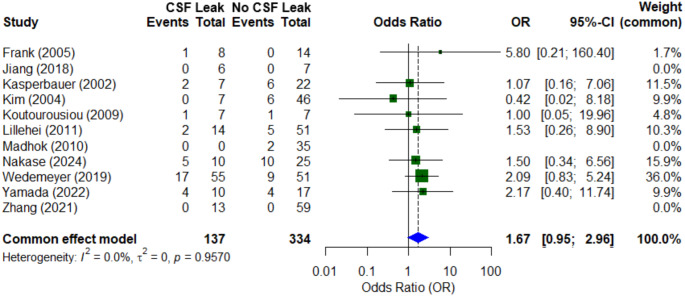
Nineteen studies, comprising 1,076 patients, were included. The overall radiological RCC recurrence rate was 19.8% over a mean follow-up of 50.4 months. The recurrence rate in closed sella surgeries was significantly higher (32.1%) than in open sellar cases (14.0%) (OR 2.28, 95% CI: 1.41-3.67, p < 0.05). Intraoperative CSF leak occurred in 29.1% of cases. Patients with CSF leaks had a higher recurrence rate (23.4% vs. 12.9%), though meta-analysis demonstrated only a non-significant trend (OR 1.67, 95% CI: 0.95-2.96). Subgroup analysis revealed that intraoperative CSF leaks were significantly associated with increased recurrence after fenestration (38.5% vs. 18.4%, p = 0.03), and cyst wall resection (21.7% vs. 7.8%, p = 0.004). In the setting of an intraoperative CSF leak, there was a trend for lower recurrence when cyst wall resection was attempted (21.7% vs. 38.5%, p = 0.09).
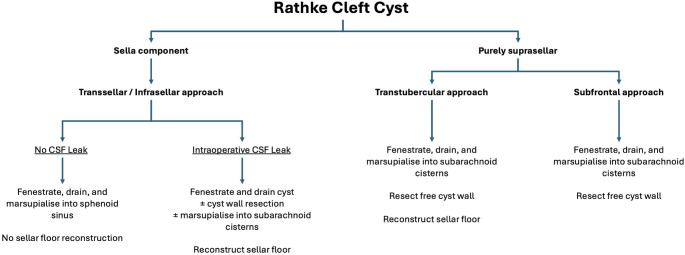
Patients undergoing transsphenoidal surgery for RCC experience high rates of postoperative radiological recurrence. Cyst fenestration while maintaining an open sellar floor (marsupialisation into the sphenoid sinus) is associated with a significantly lower risk of recurrence at over 4 years follow-up. Intraoperative CSF leaks were less strongly associated with cyst recurrence, suggesting that watertight reconstruction, rather than the leak itself, is the primary driver of reaccumulation. When a closed sella is necessitated by intraoperative CSF leak, the addition of cyst wall resection may be associated with a lower rate of recurrence than fenestration alone but must be weighed against a higher risk of AVP-deficiency.
处理拉克氏囊肿(RCC)的最佳手术技术仍不明确。经蝶窦手术后将鞍区缺损敞开(袋形缝合术)有助于囊肿内容物持续引流,但在术中发生脑脊液(CSF)漏的情况下无法进行。术中脑脊液漏和鞍底重建对RCC复发的影响需要进一步研究。
对报告经蝶窦手术后RCC复发情况的研究进行系统文献检索,并获取术中脑脊液漏发生率和颅底重建的数据。根据手术技术对研究进行分类:囊肿壁切除术与开窗术,以及开放(无重建)与闭合(重建)鞍底。
纳入19项研究,共1076例患者。平均随访50.4个月,总体影像学RCC复发率为19.8%。闭合性鞍区手术的复发率(32.1%)显著高于开放性鞍区手术(14.0%)(OR 2.28,95%CI:1.41 - 3.67,p < 0.05)。29.1%的病例发生术中脑脊液漏。脑脊液漏患者的复发率较高(23.4%对12.9%),尽管荟萃分析仅显示出不显著的趋势(OR 1.67,95%CI:0.95 - 2.96)。亚组分析显示,术中脑脊液漏与开窗术后复发增加显著相关(38.5%对18.4%,p = 0.03),以及与囊肿壁切除术后复发增加显著相关(21.7%对7.8%,p = 0.004)。在术中发生脑脊液漏的情况下,尝试进行囊肿壁切除时复发率有降低趋势(21.7%对38.5%,p = 0.09)。
接受经蝶窦手术治疗RCC的患者术后影像学复发率较高。在随访4年以上时,囊肿开窗并保持鞍底开放(袋形缝合至蝶窦)与显著较低的复发风险相关。术中脑脊液漏与囊肿复发的相关性较弱,这表明防水重建而非漏本身是囊肿重新积聚的主要驱动因素。当因术中脑脊液漏而需要进行闭合性鞍区手术时,联合囊肿壁切除可能比单纯开窗术的复发率更低,但必须权衡其导致抗利尿激素缺乏的较高风险。