Arampinyokul Ployroung, Rojananuangnit Kulawan
Department of Ophthalmology, Mettapracharak (Wat Rai Khing) Hospital, Nakhon Pathom, Thailand.
Mahidol Bumrungrak Nakhonsawan Medical Center, Nakhon Sawan, Thailand.
Clin Ophthalmol. 2025 Apr 17;19:1299-1311. doi: 10.2147/OPTH.S518659. eCollection 2025.
This study aimed to evaluate the long-term surgical outcomes of trabeculectomy with mitomycin C (MMC) and identify factors associated with surgical failure in Thai patients with primary and secondary glaucoma.
This retrospective study included 421 eyes from 397 patients with glaucoma who underwent trabeculectomy with MMC from January 1, 2012, to December 31, 2015. The patients' demographics, baseline characteristics, ocular parameters, and postoperative outcomes were analyzed. Surgical success was classified into complete success (IOP = 4-21 mmHg without anti-glaucoma medication), qualified success (IOP = 4-21 mmHg with medication), and failure (IOP >21 mmHg or <4 mmHg). Factors associated with surgical failure were assessed using Cox regression analysis.
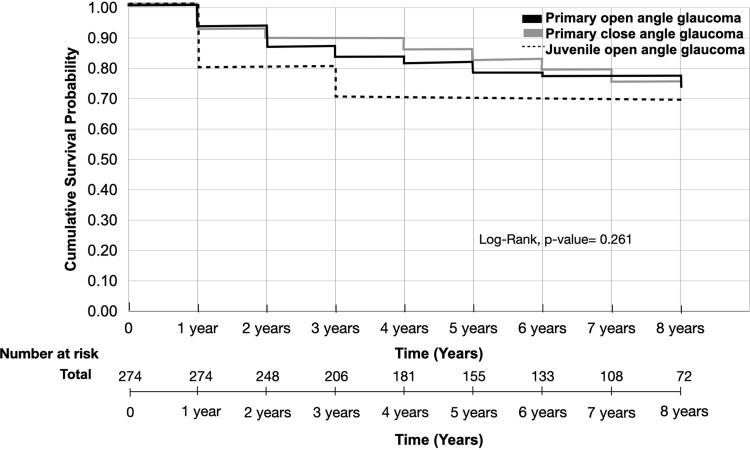
The cumulative probability of complete or qualified success at 8 years was 65.9% (95% CI: 59.9%, 71.9%); however, a significantly higher success rate was observed in the primary glaucoma group (75.1%) than in the secondary glaucoma group (47.4%) (p < 0.001). The secondary glaucoma group, particularly those with secondary closed-angle glaucoma, had the lowest success rates. Preoperative IOP, number of anti-glaucoma medications, and visual acuity were significantly different between the two groups. Etiologic factors associated with surgical failure included pseudo-exfoliation glaucoma (adjusted HR 3.23), neovascular glaucoma (adjusted HR 2.87), and secondary angle closure glaucoma (adjusted HR 2.62). Late complications were more prevalent in patients with secondary glaucoma than in those with primary glaucoma and included decreased visual acuity (5.43% vs 10.29%), hypotony (0.26% vs 1.14%), corneal decompensation (1.82% vs 3.40%), and bleb-related infection (0.19%).
Trabeculectomy with MMC remains an effective surgical option for primary glaucoma, demonstrating better long-term outcomes compared to its outcomes in patients with secondary glaucoma. Risk factors for surgical failure include specific glaucoma etiologies. These findings would personalize management strategies to optimize surgical approaches based on predictive factors for surgical success.
本研究旨在评估丝裂霉素C(MMC)小梁切除术的长期手术效果,并确定泰国原发性和继发性青光眼患者手术失败的相关因素。
这项回顾性研究纳入了2012年1月1日至2015年12月31日期间接受MMC小梁切除术的397例青光眼患者的421只眼睛。分析了患者的人口统计学、基线特征、眼部参数和术后结果。手术成功分为完全成功(眼压=4-21 mmHg,无需使用抗青光眼药物)、合格成功(眼压=4-21 mmHg,需使用药物)和失败(眼压>21 mmHg或<4 mmHg)。使用Cox回归分析评估与手术失败相关的因素。
8年时完全成功或合格成功的累积概率为65.9%(95%CI:59.9%,71.9%);然而,原发性青光眼组的成功率(75.1%)显著高于继发性青光眼组(47.4%)(p<0.001)。继发性青光眼组,尤其是继发性闭角型青光眼患者,成功率最低。两组患者术前眼压、抗青光眼药物数量和视力存在显著差异。与手术失败相关的病因因素包括剥脱性青光眼(调整后HR 3.23)、新生血管性青光眼(调整后HR 2.87)和继发性闭角型青光眼(调整后HR 2.62)。继发性青光眼患者的晚期并发症比原发性青光眼患者更常见,包括视力下降(5.43%对10.29%)、低眼压(0.26%对1.14%)、角膜失代偿(1.82%对3.40%)和滤过泡相关感染(0.19%)。
MMC小梁切除术仍然是原发性青光眼的一种有效手术选择,与继发性青光眼患者相比,其长期效果更好。手术失败的危险因素包括特定的青光眼病因。这些发现将使管理策略个性化,以根据手术成功的预测因素优化手术方法。