González-Suárez Susana, Camacho Oviedo John, Suriñach Caralt José Maria, Grao Roca Maria, Dammala Liyanage Isuru M, Pérez Lafuente Mercedes, Mena Muñoz Elisabeth, González Junyent Carla, Martínez-Martínez María, Barnés Navarro Daniel, Ruíz-Rodríguez Juan Carlos
Department of Surgery, Universitat Autònoma de Barcelona, Unitat Docent Vall d'Hebron, Pg. de la Vall d'Hebron, 119-129, 08035 Barcelona, Spain.
Department of Anesthesiology, Hospital Universitari Vall d'Hebron, Pg. de la Vall d'Hebron, 119-129, 08035 Barcelona, Spain.
J Clin Med. 2025 Apr 15;14(8):2704. doi: 10.3390/jcm14082704.
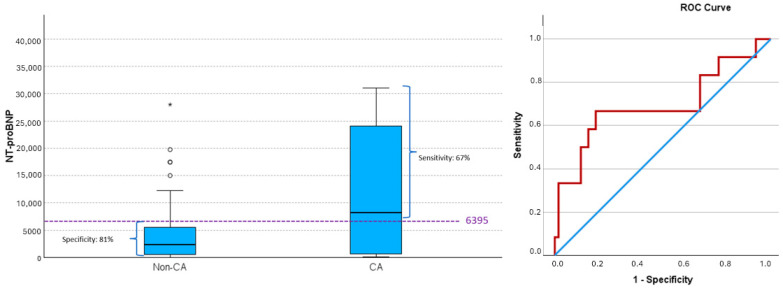
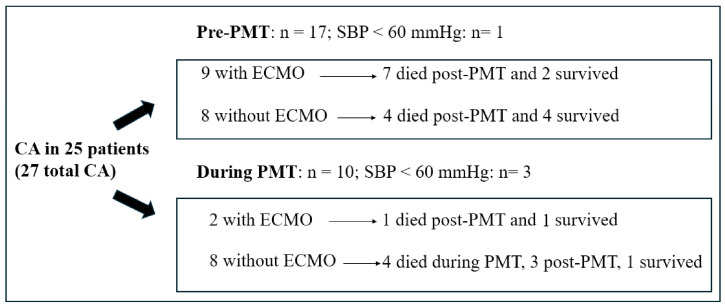
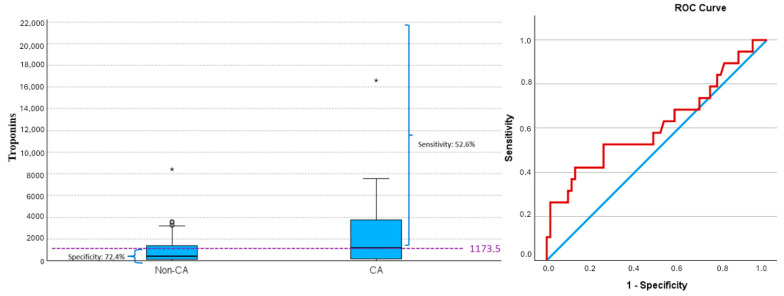
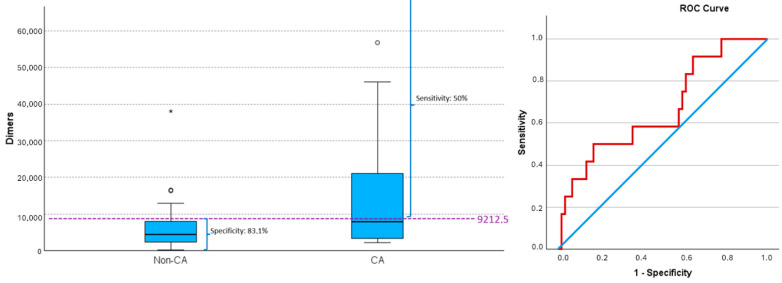
The incidence, timing, and predictors of hemodynamic and respiratory deterioration in patients with high-risk or intermediate-high-risk pulmonary embolism (PE) undergoing pulmonary mechanical thrombectomy (PMT) remain poorly understood. This hemodynamic and respiratory instability can lead to modifications in the anesthetic management. This study investigates these key factors and quantifies the 30-day mortality following thrombectomy. A retrospective study was conducted on 98 patients aged ≥18 years who underwent PMT. Patients were categorized based on the occurrence of cardiac arrest (CA). Of the 98 patients, 34 had high-risk PE, 62 intermediate/high-risk, and 2 low risk. There were 27 cases of CA, 17 pre- and 10 intra-PMT. An SBP < 90 mmHg increases the risk of CA by 33 ( < 0.001); men have an 8-fold higher risk than women ( = 0.004); SpO <90% by 6 ( = 0.012); and pre-existing respiratory conditions increase the risk by 4 ( = 0.047)). N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels were 8206 ± 11660.86 and 2388.50 ± 5683.71 pg/mL ( = 0.035) in patients with and without CA, respectively. During PMT, 14% of patients required increased vasoactive drug use, and 38.77% were intubated, including 12 who required ECMO support. Sedation was administered in 64.3% of patients, while general anesthesia was used in 38.8%, with a preemptive indication in 23.5%. The survival rate of patients without CA before and/or during PMT was 96%. While PMT was successfully performed in all patients, hemodynamic and respiratory instability remained a significant concern. More than 10% of patients experienced severe hemodynamic instability, primarily during thrombus extraction, requiring conversion from sedation to general anesthesia. Male sex, pre-existing respiratory disease, SpO < 90%, and SBP < 90 mmHg were associated with an increased risk of CA. Additionally, elevated NT-proBNP levels were linked to a higher incidence of CA.
对于接受肺机械血栓切除术(PMT)的高危或中高危肺栓塞(PE)患者,血流动力学和呼吸功能恶化的发生率、发生时间及预测因素仍知之甚少。这种血流动力学和呼吸功能不稳定可导致麻醉管理的调整。本研究调查了这些关键因素,并对血栓切除术后30天死亡率进行了量化。对98例年龄≥18岁接受PMT的患者进行了一项回顾性研究。根据心脏骤停(CA)的发生情况对患者进行分类。98例患者中,34例为高危PE,62例为中/高危,2例为低风险。发生27例CA,17例发生在PMT前,10例发生在PMT术中。收缩压(SBP)<90 mmHg使CA风险增加33倍(P<0.001);男性发生CA的风险是女性的8倍(P = 0.004);血氧饱和度(SpO₂)<90%使CA风险增加6倍(P = 0.012);既往有呼吸系统疾病使CA风险增加4倍(P = 0.047)。发生和未发生CA的患者N末端B型脑钠肽原(NT-proBNP)水平分别为8206±11660.86和2388.50±5683.71 pg/mL(P = 0.0