Zhou Yumin, Wu Fan, Deng Zhishan, Wang Zihui, Tian Heshen, Huang Peiyu, Zheng Youlan, Yang Huajing, Zhao Ningning, Dai Cuiqiong, Yang Changli, Yu Shuqing, Tian Jia, Cui Jiangyu, Liu Shengming, Wang Dali, Wang Xiaoping, Lu Jiachun, Zhong Nanshan, Ran Pixin
State Key Laboratory of Respiratory Disease & National Clinical Research Center for Respiratory Disease & National Center for Respiratory Medicine & Guangzhou Institute of Respiratory Health, The First Affiliated Hospital of Guangzhou Medical University, 195 Dongfeng Xi Road, Guangzhou, 510120, China.
Guangzhou National Laboratory, Guangzhou, China.
Respir Res. 2025 Apr 28;26(1):169. doi: 10.1186/s12931-025-03244-3.
Small airway dysfunction (SAD) is common but little is known about the longitudinal prognosis of spirometry-defined SAD. Therefore, we aimed to evaluate the risk of lung function decline and incident chronic obstructive pulmonary disease (COPD) of spirometry-defined SAD.
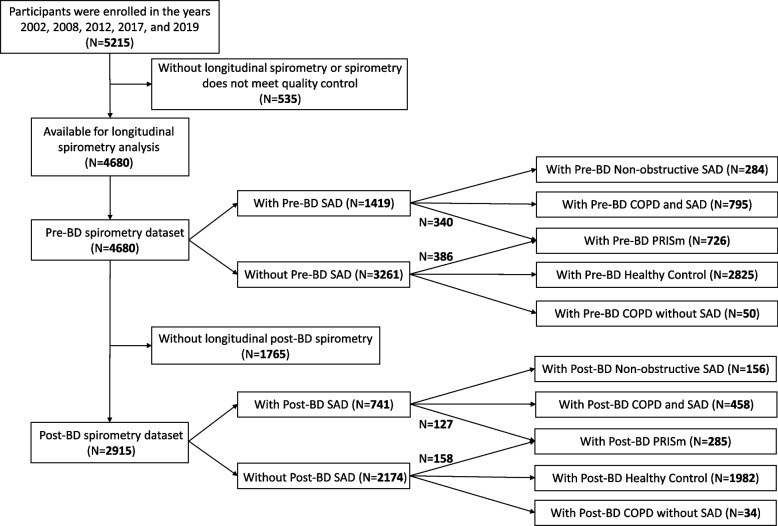
It was a population-based prospective cohort study conducted in Guangdong, China. Participants were enrolled in the years 2002, 2008, 2012, 2017, and 2019, and those who completed baseline demographic data, a standardized epidemiological questionnaire for COPD, and spirometry were included. Follow-up visits were conducted every three years after enrolment, with a maximum follow-up time of 15 years and a minimum follow-up time of 3 years. Spirometry-defined SAD was defined as having at least two out of three parameters (maximal mid-expiratory flow, forced expiratory flow 50%, and forced expiratory flow 75%) below 65% of the predicted value. Non-obstructive SAD and obstructive SAD were further differentiated based on the presence of airflow obstruction (forced expiratory volume in one second [FEV]/forced vital capacity [FVC] < 0.70). Pre- and post-bronchodilator spirometry measurements were analyzed separately.
Pre-bronchodilator spirometry dataset included 4680 participants (mean age 55.3 [10.8] years, 2194 [46.9%] males). Participants with pre-bronchodilator SAD had a significantly faster annual decline of FEV % of predicted value (0.31 ± 0.05 vs. 0.20 ± 0.03 %/year; difference: 0.12 [95% confidence interval: 0.01-0.23]; P = 0.023), FVC, and FVC % of predicted value compared to those without pre-bronchodilator SAD. The annual decline of lung function in participants with pre-bronchodilator non-obstructive SAD was not significantly different from that in pre-bronchodilator healthy controls, but they were more likely to progress to spirometry-defined COPD (adjusted hazard ratio: 2.92 [95% confidence interval: 2.28-3.76], P < 0.001). Post-bronchodilator spirometry dataset yielded similar results.
Individuals with spirometry-defined SAD have a faster decline in lung function compared to those without SAD, and non-obstructive SAD is more likely to progress to spirometry-defined COPD.
Chinese Clinical Trials Registration ChiCTR1900024643. Registered on 19 July 2019.
小气道功能障碍(SAD)很常见,但对于肺量计定义的SAD的纵向预后知之甚少。因此,我们旨在评估肺量计定义的SAD患者肺功能下降和发生慢性阻塞性肺疾病(COPD)的风险。
这是一项在中国广东进行的基于人群的前瞻性队列研究。参与者于2002年、2008年、2012年、2017年和2019年入组,纳入那些完成基线人口统计学数据、COPD标准化流行病学调查问卷和肺量计检查的患者。入组后每三年进行一次随访,最长随访时间为15年,最短随访时间为3年。肺量计定义的SAD定义为三个参数(最大呼气中期流速、用力呼气流量50%和用力呼气流量75%)中至少有两个低于预测值的[具体数值]。根据是否存在气流受限(一秒用力呼气容积[FEV]/用力肺活量[FVC]<0.70)进一步区分非阻塞性SAD和阻塞性SAD。分别分析支气管扩张剂使用前和使用后的肺量计测量结果。
支气管扩张剂使用前的肺量计数据集包括4680名参与者(平均年龄55.3[10.8]岁,2194[46.9%]为男性)。与无支气管扩张剂使用前SAD的参与者相比,有支气管扩张剂使用前SAD的参与者预测值的FEV%年下降率显著更快(0.31±0.05 vs.0.20±0.03%/年;差异:0.12[95%置信区间:0.01 - 0.23];P = 0.023),FVC以及预测值的FVC%年下降率也更快。支气管扩张剂使用前非阻塞性SAD参与者的肺功能年下降率与支气管扩张剂使用前健康对照组无显著差异,但他们更有可能进展为肺量计定义的COPD(调整后风险比:2.92[95%置信区间:2.28 - 3.76],P<0.001)。支气管扩张剂使用后的肺量计数据集得出了类似结果。
与无SAD的个体相比,肺量计定义的SAD个体的肺功能下降更快,且非阻塞性SAD更有可能进展为肺量计定义的COPD。
中国临床试验注册中心ChiCTR1900024643。于2019年7月19日注册。