Räuber Saskia, Schulte-Mecklenbeck Andreas, Sarink Kelvin, Müller Christoph, Mannil Manoj, Langenbruch Lisa, Dik Andre, Barman Sumanta, Strippel Christine, Gallus Marco, Golombeck Kristin S, Schroeter Christina B, Willison Alice, Nelke Christopher, Ismail Fatme Seval, Schwindt Wolfram, Goebels Norbert, Kovac Stjepana, Wiendl Heinz, Meyer Zu Hörste Gerd, Duning Thomas, Hanke Michael, Ruck Tobias, Heindel Walter, Dannlowski Udo, Hahn Tim, Gross Catharina C, Meuth Sven G, Melzer Nico
Department of Neurology with Institute of Translational Neurology, University of Münster, Münster 48149, Germany.
Department of Neurology, Medical Faculty and University Hospital Düsseldorf, Heinrich Heine University of Düsseldorf, Düsseldorf 40225, Germany.
Brain Commun. 2025 Apr 18;7(2):fcaf156. doi: 10.1093/braincomms/fcaf156. eCollection 2025.
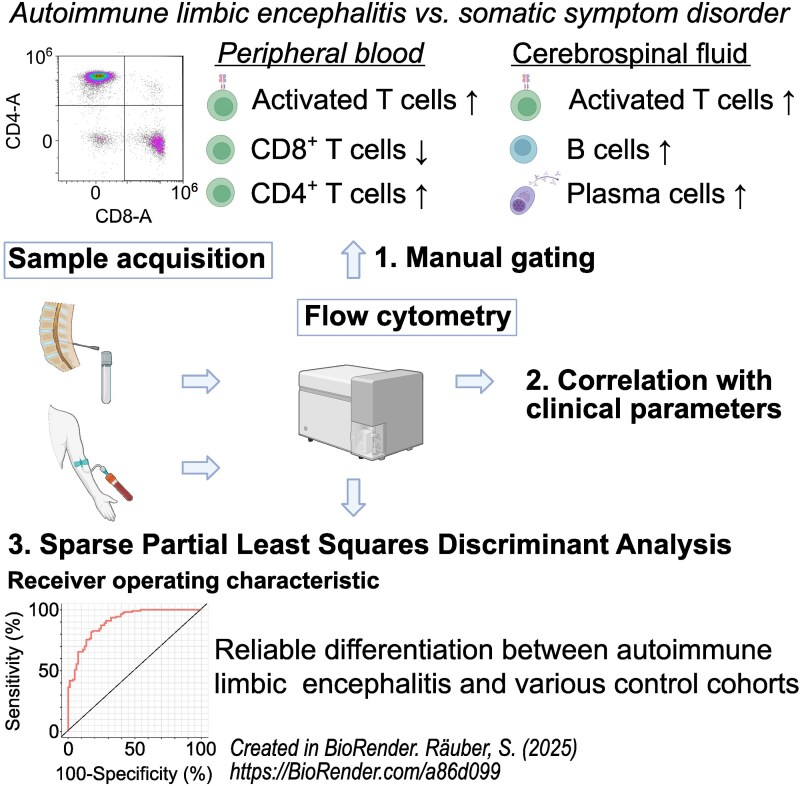
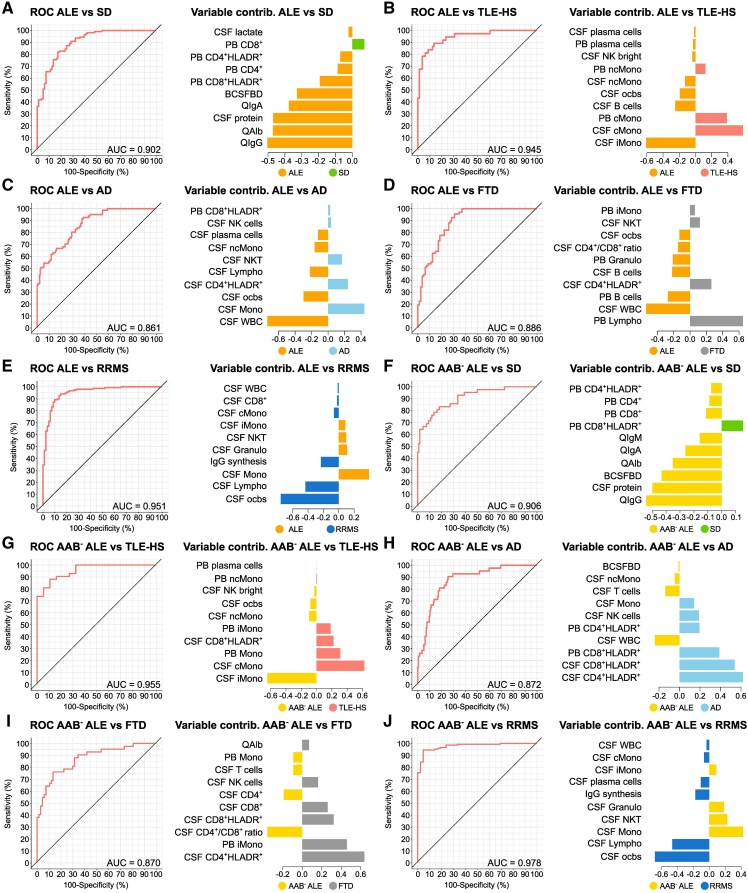
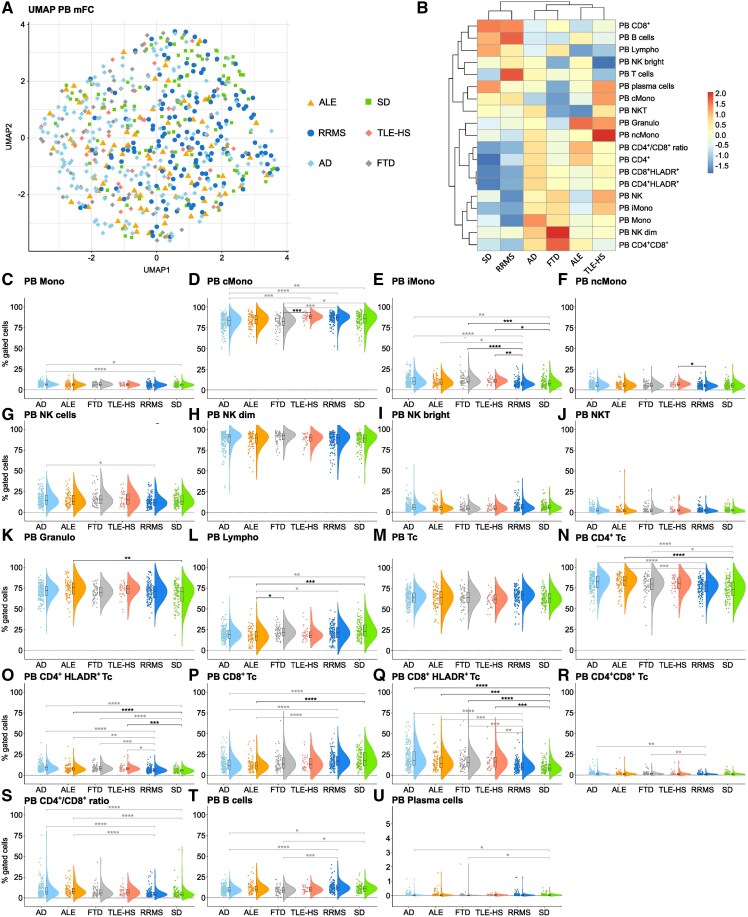
Autoimmune limbic encephalitis is an inflammatory condition confined to the limbic system of the brain that is deemed to be due to a dysregulated immune response. However, the exact pathophysiological mechanisms remain elusive. Diagnosis of autoimmune limbic encephalitis currently relies on clinical consensus criteria. However, diagnostic workup can be challenging, potentially delaying treatment initiation associated with poor clinical outcomes. We retrospectively identified 640 patients (81 autoimmune limbic encephalitis, 148 relapsing-remitting multiple sclerosis, 197 Alzheimer's disease, 67 frontotemporal dementia, 37 temporal lobe epilepsy with hippocampal sclerosis and 110 somatic symptom disorder patients). Applying multidimensional flow-cytometry together with novel computational approaches, we analysed the peripheral blood and cerebrospinal fluid immune cell profiles at different disease stages and performed correlations with clinical parameters (i.e. neuropsychological performance, EEG and MRI). We were able to identify a shared immune signature of autoimmune limbic encephalitis showing similarities in adaptive B and T cell response with other inflammatory central nervous system diseases and in T cell patterns with neurodegenerative disorders. Antibody-negative autoimmune limbic encephalitis showed a pronounced T cell response in peripheral blood similar to temporal lobe epilepsy and hippocampal sclerosis and neurodegenerative disorders differentiating from antibody-positive autoimmune limbic encephalitis and classical inflammatory central nervous system diseases with regard to B and plasma cell response. Longitudinal immune cell phenotyping in autoimmune limbic encephalitis revealed dynamic changes over time mainly affecting the innate, B and plasma cell compartment. Correlation analysis indicated associations between the baseline immune cell profile, especially lymphocytes, and neuropsychological performance, as well as EEG and MRI abnormalities. Applying novel computational approaches, we found that multidimensional flow cytometry together with routine CSF parameters could reliably distinguish autoimmune limbic encephalitis from controls and clinical differential diagnoses. Incorporation of multidimensional flow cytometry parameters showed superior discriminatory ability compared with CSF routine parameters alone. Taken together, autoimmune limbic encephalitis is characterized by a B and T cell dominated intrathecal immune-cell signature corresponding to changes reported in the brain parenchyma and showing similarities with classical inflammatory central nervous system diseases and neurodegenerative disorders. Incorporating clinical parameters and applying novel computational approaches, we could show that multidimensional flow cytometry might be a beneficial complement to the established diagnostic workup of autoimmune limbic encephalitis promoting early diagnosis and facilitating outcome prediction to enhance individualized treatment regimes.
自身免疫性边缘叶脑炎是一种局限于大脑边缘系统的炎症性疾病,被认为是由于免疫反应失调所致。然而,确切的病理生理机制仍不清楚。目前,自身免疫性边缘叶脑炎的诊断依赖于临床共识标准。然而,诊断检查可能具有挑战性,可能会延迟治疗的开始,从而导致不良的临床结果。我们回顾性地确定了640例患者(81例自身免疫性边缘叶脑炎、148例复发缓解型多发性硬化症、197例阿尔茨海默病、67例额颞叶痴呆、37例伴有海马硬化的颞叶癫痫和110例躯体症状障碍患者)。应用多维流式细胞术和新的计算方法,我们分析了不同疾病阶段外周血和脑脊液中的免疫细胞谱,并与临床参数(即神经心理学表现、脑电图和磁共振成像)进行了相关性分析。我们能够识别出自身免疫性边缘叶脑炎的一种共同免疫特征,其在适应性B细胞和T细胞反应方面与其他炎症性中枢神经系统疾病相似,在T细胞模式方面与神经退行性疾病相似。抗体阴性的自身免疫性边缘叶脑炎在外周血中表现出明显的T细胞反应,类似于颞叶癫痫和海马硬化以及神经退行性疾病,在B细胞和浆细胞反应方面与抗体阳性的自身免疫性边缘叶脑炎和经典炎症性中枢神经系统疾病不同。自身免疫性边缘叶脑炎的纵向免疫细胞表型分析显示,随着时间的推移会发生动态变化,主要影响固有免疫细胞、B细胞和浆细胞区室。相关性分析表明,基线免疫细胞谱,尤其是淋巴细胞,与神经心理学表现以及脑电图和磁共振成像异常之间存在关联。应用新的计算方法,我们发现多维流式细胞术与常规脑脊液参数相结合能够可靠地将自身免疫性边缘叶脑炎与对照及临床鉴别诊断区分开来。与单独的脑脊液常规参数相比,纳入多维流式细胞术参数显示出更好的鉴别能力。综上所述,自身免疫性边缘叶脑炎的特征是鞘内免疫细胞特征以B细胞和T细胞为主,这与脑实质中报道的变化相对应,并且与经典炎症性中枢神经系统疾病和神经退行性疾病相似。结合临床参数并应用新的计算方法,我们可以证明多维流式细胞术可能是对已确立的自身免疫性边缘叶脑炎诊断检查的有益补充,有助于早期诊断并促进结果预测,以加强个体化治疗方案。