Zhang Bicheng, Song Yuxiao, Min Qian, Cheng Weiting, Wang Jun, Fu Yang, Yin Jiaxin
Cancer Center, Renmin Hospital of Wuhan University, Wuhan, China.
Department of Oncology, The First Affiliated Hospital of Shandong First Medical University, Jinan, China.
Front Immunol. 2025 Apr 28;16:1579420. doi: 10.3389/fimmu.2025.1579420. eCollection 2025.
Immune checkpoint inhibitors (ICIs) combined with chemotherapy have become a standard first-line treatment for advanced non-small cell lung cancer (NSCLC). However, the optimal sequence of administrating the two treatments remains controversial.
This study included advanced NSCLC patients who received ICIs combined with chemotherapy at Renmin Hospital of Wuhan University and Xiangyang Hospital, Hubei University of Chinese Medicine between 1st September 2020 and 30th September 2024. Patients were categorized into the concurrent, immune-chemo, and chemo-immune groups based on different sequences of treatment administration. The primary endpoints evaluated were survival and treatment efficacy. The secondary endpoint assessed was treatment-related adverse events (TRAEs).
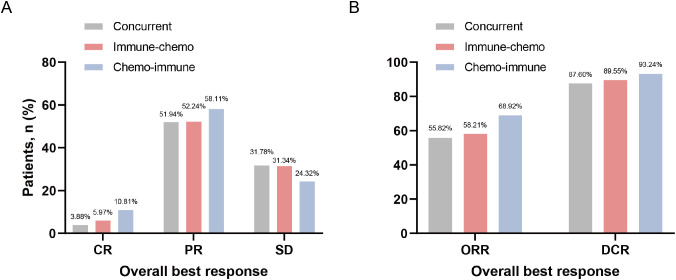
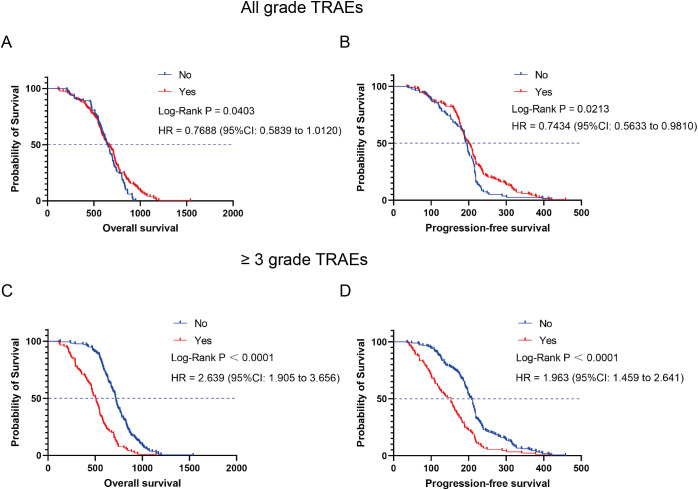
This two-center, retrospective study included 270 NSCLC patients who received ICIs plus chemotherapy. Survival analysis revealed statistically significant differences across treatment groups. The median overall survival (mOS) durations were 636 days (concurrent group), 615 days (immune-chemo group), and 749 days (chemo-immune group), with a log-rank test demonstrating significant intergroup differences ( = 0.0017). Similarly, median progression-free survival (mPFS) showed distinct patterns at 178 days, 180 days, and 216 days for the respective groups (log-rank = 0.0134). Additionally, the objective response rates (ORRs) for the three groups were 55.82% (72/129), 58.21% (39/67), and 68.92% (51/74), respectively. The incidence of TRAEs of any grade in the concurrent, the immune-chemo, and the chemo-immune groups was 77.52% (100/129), 65.67% (44/67), and 59.46% (44/74) rates, respectively, which was a significant difference (χ²=7.91, =0.019). Despite patients experiencing Grade 3 or higher TRAEs had extremely poor prognoses, overall, patients who developed any grade of TRAEs had better survival outcomes, particularly those with skin or endocrine toxicity.
These findings suggest that the administration sequence of chemotherapy followed by ICIs may yield the greatest clinical benefit, providing a basis for clinical decision-making.
免疫检查点抑制剂(ICIs)联合化疗已成为晚期非小细胞肺癌(NSCLC)的标准一线治疗方案。然而,两种治疗的最佳给药顺序仍存在争议。
本研究纳入了2020年9月1日至2024年9月30日期间在武汉大学人民医院和湖北中医药大学附属襄阳医院接受ICIs联合化疗的晚期NSCLC患者。根据不同的治疗给药顺序,将患者分为同步治疗组、免疫化疗组和化疗免疫组。评估的主要终点为生存率和治疗疗效。评估的次要终点为治疗相关不良事件(TRAEs)。
这项两中心回顾性研究纳入了270例接受ICIs加化疗的NSCLC患者。生存分析显示各治疗组之间存在统计学显著差异。中位总生存期(mOS)分别为636天(同步治疗组)、615天(免疫化疗组)和749天(化疗免疫组),对数秩检验显示组间差异显著(=0.0017)。同样,中位无进展生存期(mPFS)在各组中分别为178天、180天和216天,呈现出不同模式(对数秩=0.0134)。此外,三组的客观缓解率(ORRs)分别为55.82%(72/129)、58.21%(39/67)和68.92%(51/74)。同步治疗组、免疫化疗组和化疗免疫组任何级别的TRAEs发生率分别为77.52%(100/129)、65.67%(44/67)和59.46%(44/74),差异有统计学意义(χ²=7.91,=0.019)。尽管发生3级或更高级别TRAEs的患者预后极差,但总体而言,发生任何级别的TRAEs的患者生存结局更好,尤其是那些有皮肤或内分泌毒性的患者。
这些发现表明,先进行化疗再使用ICIs的给药顺序可能产生最大的临床获益,为临床决策提供了依据。