Liu Yin, Guo Xiaoli, Xu Huifang, Wang Xiaoyang, Liu Hongwei, Wang Hong, Kang Ruihua, Chen Qiong, Qie Ranran, Zhao Mengfei, Cheng Cheng, Zheng Liyang, Liu Shuzheng, Qiao Youlin, Zhang Shaokai
Department of Cancer Epidemiology, The Affiliated Cancer Hospital of Zhengzhou University & Henan Cancer Hospital, Zhengzhou, 450008, China.
Center for Global Health, School of Population Medicine and Public Health, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100005, China.
BMC Public Health. 2025 May 15;25(1):1783. doi: 10.1186/s12889-025-22977-w.
Lung cancer is the leading cause of cancer-related deaths worldwide, with non-smokers in China accounting for over 40% of cases. Despite the proven efficacy of low-dose computed tomography (LDCT) in early detection and reduction of lung cancer mortality, the current paradigm of lung cancer screening, heavily focused on smoking status and age, may inadequately address the unique risk factors associated with non-smokers, particularly those with a family history of the disease. This study evaluates the cost-effectiveness of LDCT screening for non-smokers with a first-degree relative (FDR) history of lung cancer, a group at particularly high-risk.
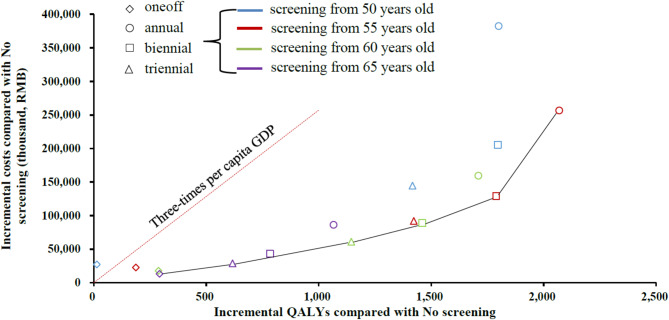
We developed a state-transition Markov model to evaluate the incremental cost-effectiveness ratios (ICERs) of 16 screening strategies for a hypothetical cohort of 100,000 non-smoking individuals aged 50 with a FDR history of lung cancer, considering various starting ages (50, 55, 60, 65 years) and intervals (one-off, annual, biennial, triennial). The willingness-to-pay (WTP) threshold was set at three times China's 2022 per-capita GDP. Sensitivity analyses, scenario analyses and subgroup analysis by sex, were conducted.
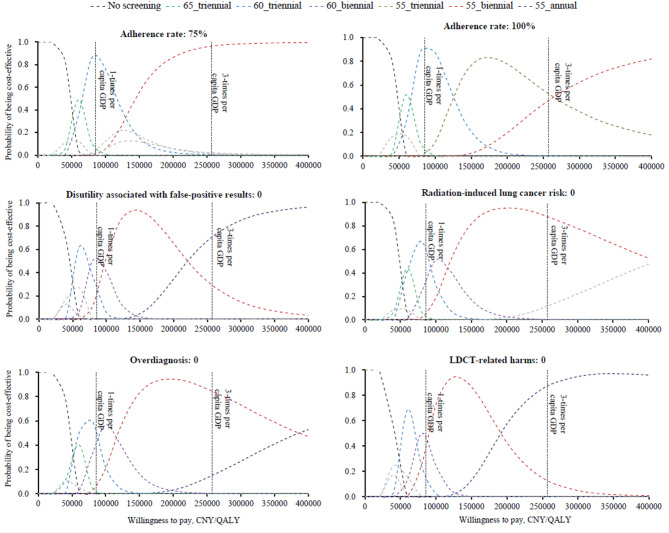
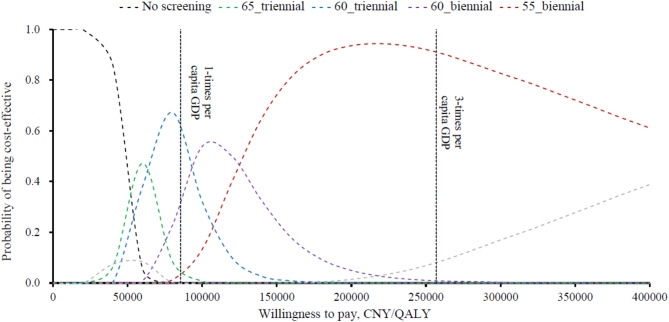
Compared to no screening, all strategies except one-off screening at age 50, were cost-effective for both sexes. Biennial LDCT starting at age 55 was found to be most effective, with an ICER of CNY 68,932/QALY for males, and CNY 80,056/QALY for females. This cost-effectiveness probability for this strategy was approximately 90% for both sexes. Sensitivity analyses indicated that annual screening at age 55 was optimal without discounting. For males, biennial at age 60 was optimal if the FDR-related odds ratio for lung cancer incidence was below 1.492. Triennial screening at age 55 was optimal for females at full adherence. Ignoring disutility from false-positive results, annual at age 55 was optimal for both sexes.
LDCT screening for non-smokers with a FDR history of lung cancer is cost-effective, especially biennial screening at 55. These findings support the development of more inclusive screening guidelines, which could enhance early detection and reduce mortality rates.
肺癌是全球癌症相关死亡的主要原因,在中国,非吸烟者患肺癌的病例占比超过40%。尽管低剂量计算机断层扫描(LDCT)在肺癌早期检测和降低死亡率方面的疗效已得到证实,但目前肺癌筛查模式主要侧重于吸烟状况和年龄,可能无法充分应对与非吸烟者相关的独特风险因素,尤其是那些有肺癌家族病史的人。本研究评估了对有肺癌一级亲属(FDR)病史的非吸烟者进行LDCT筛查的成本效益,这是一个特别高危的群体。
我们建立了一个状态转换马尔可夫模型,以评估针对100000名50岁有肺癌FDR病史的非吸烟个体的假设队列的16种筛查策略的增量成本效益比(ICER),考虑了不同的起始年龄(50、55、60、65岁)和筛查间隔(一次性、每年、每两年、每三年)。支付意愿(WTP)阈值设定为中国2022年人均GDP的三倍。进行了敏感性分析、情景分析以及按性别进行的亚组分析。
与不进行筛查相比,除50岁一次性筛查外,所有策略对男女均具有成本效益。发现从55岁开始每两年进行一次LDCT筛查最为有效,男性的ICER为68932元/QALY,女性为80056元/QALY。该策略对男女的成本效益概率均约为90%。敏感性分析表明,55岁时每年进行筛查在不考虑贴现的情况下是最优的。对于男性,如果肺癌发病的FDR相关优势比低于1.492,则60岁时每两年筛查一次是最优的。在完全依从的情况下,55岁时每三年进行一次筛查对女性是最优的。忽略假阳性结果带来的负效用,55岁时每年进行筛查对男女都是最优的。
对有肺癌FDR病史的非吸烟者进行LDCT筛查具有成本效益,尤其是55岁时每两年进行一次筛查。这些发现支持制定更具包容性的筛查指南,这可以提高早期检测率并降低死亡率。