Wallace Beth I, Cohen-Mekelburg Shirley, Van Tony, Lipson Rachel, Kenney Brooke, Tatchin Chelsea, Baker Jessica, Saini Sameer D, Waljee Akbar K
Center for Clinical Management Research, VA Ann Arbor Health Care System, Ann Arbor, MI, USA.
Department of Internal Medicine, VA Ann Arbor Health Care System, Ann Arbor, MI, USA.
Commun Med (Lond). 2025 May 18;5(1):184. doi: 10.1038/s43856-025-00869-9.
Glucocorticoids are used commonly despite their toxicity and availability of effective alternatives. Prior claims-based studies evaluating effect of clinician specialty on glucocorticoid prescribing do not examine how facility-level resources affect prescribing patterns. We aim to describe the effect of facility complexity and clinician specialty on oral glucocorticoid prescribing in the general population.
This is a national cross-sectional study of Veterans prescribed oral glucocorticoids during 2021-2022. We defined glucocorticoid use as ≥1 outpatient pharmacy claim for oral glucocorticoids, and prolonged use as ≥30 days' supply dispensed within 365 days. We defined complexity, rurality, and region using VHA operational metrics, and clinician specialty using NUCC taxonomy codes. We descriptively evaluated demographics, comorbidities, and healthcare utilization stratified by glucocorticoid use. We calculated the proportion of users and prolonged users at each facility, stratified by complexity, rurality, and region. We calculated the proportion of glucocorticoid prescriptions by clinician specialty. For three high-prescribing specialties, we calculated the facility-level proportion of glucocorticoid prescriptions by complexity designation.
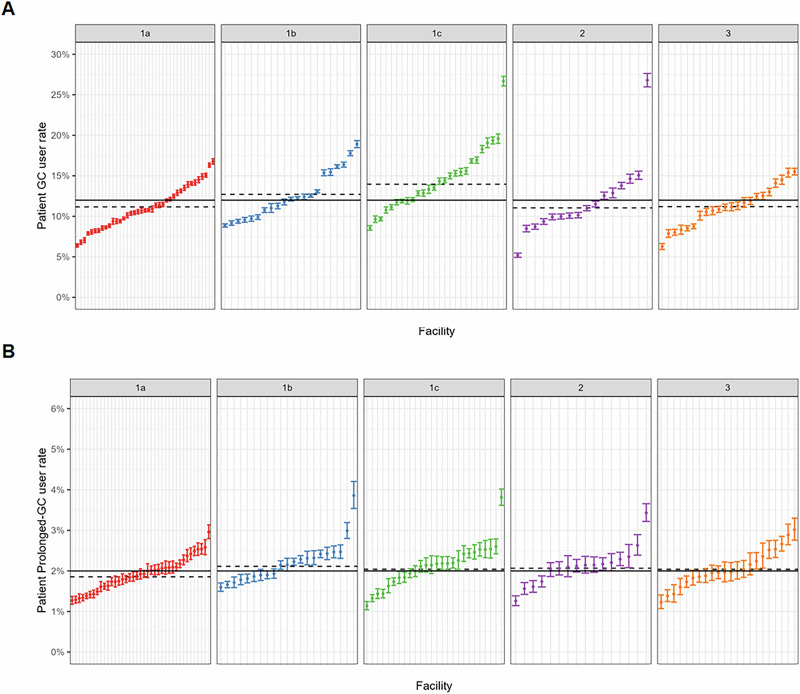
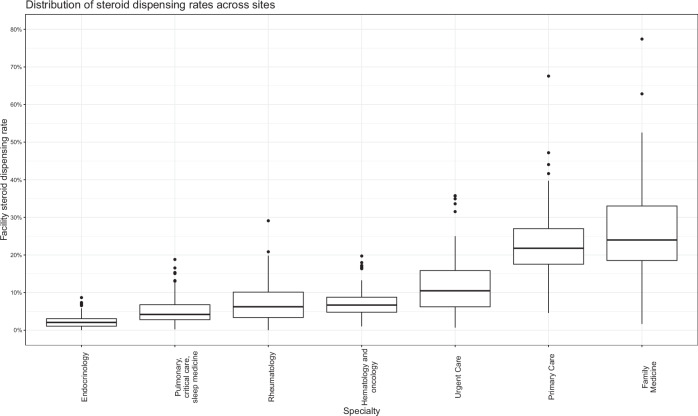
Here we show that among 5,729,134 patients at 124 facilities, a mean of 12.1% (SD 3.5%) are glucocorticoid users; 2.1% (SD 0.5%) were prolonged users. Rates of use and prescribing vary substantially within and across facility complexity designations. Family practice represents 18.8% of glucocorticoid-prescribing clinicians but prescribes 26.3% of filled prescriptions. Family practice displays higher prescribing at lower-complexity sites.
In this large national population, overall and prolonged glucocorticoid use are common and prescribing patterns vary by clinician type and complexity designation. Clinician-facing interventions to address knowledge gaps, incentivize non-glucocorticoid treatments, or facilitate specialty care access may reduce overuse among high-prescribing clinicians.
尽管糖皮质激素有毒性且有有效的替代药物,但仍被广泛使用。先前基于索赔的研究评估临床医生专业对糖皮质激素处方的影响时,未考察机构层面的资源如何影响处方模式。我们旨在描述机构复杂性和临床医生专业对普通人群口服糖皮质激素处方的影响。
这是一项对2021年至2022年期间开具口服糖皮质激素处方的退伍军人进行的全国性横断面研究。我们将糖皮质激素的使用定义为门诊药房至少有1次口服糖皮质激素的索赔记录,长期使用定义为在365天内发放的药物供应量≥30天。我们使用退伍军人健康管理局(VHA)的运营指标定义复杂性、农村地区和地区,使用国家统一收费委员会(NUCC)分类代码定义临床医生专业。我们按糖皮质激素使用情况对人口统计学、合并症和医疗保健利用情况进行了描述性评估。我们计算了每个机构中使用者和长期使用者的比例,并按复杂性、农村地区和地区进行分层。我们计算了按临床医生专业划分的糖皮质激素处方比例。对于三个高处方量的专业,我们按复杂性指定计算了机构层面的糖皮质激素处方比例。
我们发现,在124个机构的5,729,134名患者中,平均有12.1%(标准差3.5%)是糖皮质激素使用者;2.1%(标准差0.5%)是长期使用者。在不同机构复杂性指定范围内和之间,使用率和处方率差异很大。家庭医学医生占开具糖皮质激素处方临床医生的18.8%,但开具的已配药处方占26.3%。家庭医学在复杂性较低的机构中处方量更高。
在这个庞大的全国性人群中,糖皮质激素的总体使用和长期使用很常见,处方模式因临床医生类型和复杂性指定而异。针对临床医生的干预措施,以解决知识差距、激励非糖皮质激素治疗或促进专科护理的获取,可能会减少高处方量临床医生的过度使用。