Bao Wuyongga, Zeng Keyu, Huang Jiayan, Yu Boyang, Gou Zehui, Lu Qiang
Department of Medical Ultrasound, West China Hospital, Sichuan University, Chengdu, China.
Quant Imaging Med Surg. 2025 May 1;15(5):4375-4386. doi: 10.21037/qims-2024-2670. Epub 2025 Apr 28.
Pancreatic cancer is highly lethal and often diagnosed at an advanced stage, highlighting the need for early and accurate diagnosis. Although imaging plays a crucial role, definitive pathological confirmation requires biopsy. Percutaneous ultrasound-guided core needle biopsy (US-CNB), computed tomography-guided core needle biopsy (CT-CNB), and endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) are the three main biopsy techniques, each differing in diagnostic accuracy, safety, and cost-effectiveness. The aim of this study was to compare the diagnostic value, safety, and cost-effectiveness of these three biopsy techniques for suspiciously malignant pancreatic lesions.
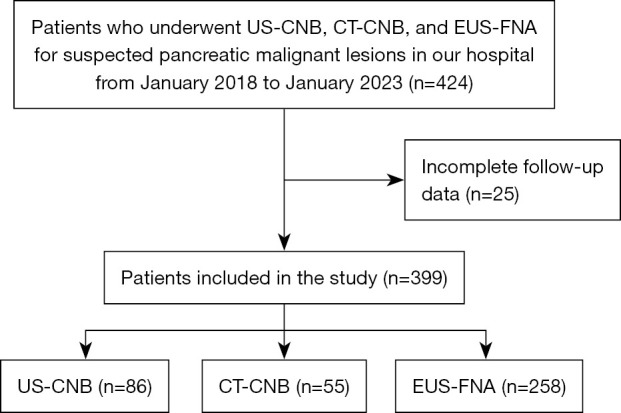
We retrospectively evaluated patients with suspicious malignant pancreatic lesions who underwent US-CNB, CT-CNB, or EUS-FNA from January 2018 to January 2023. We compared technical success rates, sample adequacy, diagnostic accuracy, sensitivity, specificity, and complication rates of three groups. Additionally, we calculated the cost/effectiveness ratio (C/E) and incremental cost-effectiveness ratio (ICER) for each method.
A total of 399 patients were enrolled (US-CNB, n=86; CT-CNB, n=55; EUS-FNA, n=258), achieving 100% technical success. Sample adequacy satisfaction rates were 97.70% for US-CNB, 90.90% for CT-CNB, and 74.03% for EUS-FNA, with EUS-FNA significantly lower compared to the other two methods (P<0.001). Diagnostic accuracy was significantly higher for US-CNB (97.70%) and CT-CNB (90.90%) compared to EUS-FNA (69.80%) (P<0.001). Complication rates were 15.12% for US-CNB, 16.36% for CT-CNB, and 10.47% for EUS-FNA, with no significant differences (P=0.319). Compared to EUS-FNA, ICER for US-CNB was -14,367.7 yuan and for CT-CNB was -8,279.22 yuan per correct diagnosis, both below the willingness-to-pay threshold.
US-CNB and CT-CNB demonstrate superior diagnostic accuracy and specimen adequacy compared to EUS-FNA for suspected malignant pancreatic lesions. There are no significant differences in postoperative complication rates among three biopsy methods. In terms of cost-effectiveness, US-CNB and CT-CNB have lower costs and higher effectiveness than EUS-FNA, indicating greater economic efficiency.
胰腺癌具有高度致死性,且常于晚期被诊断出来,这凸显了早期准确诊断的必要性。尽管影像学起着关键作用,但明确的病理确诊需要活检。经皮超声引导下的粗针活检(US-CNB)、计算机断层扫描引导下的粗针活检(CT-CNB)和内镜超声引导下的细针穿刺抽吸活检(EUS-FNA)是三种主要的活检技术,它们在诊断准确性、安全性和成本效益方面各有不同。本研究的目的是比较这三种活检技术对可疑恶性胰腺病变的诊断价值、安全性和成本效益。
我们回顾性评估了2018年1月至2023年1月期间接受US-CNB、CT-CNB或EUS-FNA检查的可疑恶性胰腺病变患者。我们比较了三组的技术成功率、样本充足率、诊断准确性、敏感性、特异性和并发症发生率。此外,我们计算了每种方法的成本/效益比(C/E)和增量成本效益比(ICER)。
共纳入399例患者(US-CNB组86例;CT-CNB组55例;EUS-FNA组258例),技术成功率均达到100%。US-CNB的样本充足满意度为97.70%,CT-CNB为90.90%,EUS-FNA为74.03%,EUS-FNA明显低于其他两种方法(P<0.001)。与EUS-FNA(69.80%)相比,US-CNB(97.70%)和CT-CNB(90.90%)的诊断准确性明显更高(P<0.001)。US-CNB的并发症发生率为15.12%,CT-CNB为16.36%,EUS-FNA为10.47%,无显著差异(P=0.319)。与EUS-FNA相比,US-CNB的ICER为每例正确诊断-14,367.7元,CT-CNB为-8,279.22元,均低于支付意愿阈值。
对于可疑恶性胰腺病变,与EUS-FNA相比,US-CNB和CT-CNB显示出更高的诊断准确性和样本充足率。三种活检方法术后并发症发生率无显著差异。在成本效益方面,US-CNB和CT-CNB比EUS-FNA成本更低、效益更高,表明具有更高的经济效率。