Cantinotti Massimiliano, Voges Inga, di Salvo Giovanni, Ortiz-Garrido Almudena, Bharucha Tara, Grotenhuis Heynric, Sabate-Rotes Anna, Cavigelli Anna, Roest Arno, Sendzikaite Skaiste, Nolan Oscar, Ramcharan Tristan, Koubsky Karel, Brun Henrik, Petropoulos Andreas C, Bellsham-Revell Hannah, Kaneva-Nencheva Anna, Dinarevic Senka Mesihovic, Abumehdi Mohammad Ryan, Óskarsson Gylfi, Olejnik Peter, Doros Gabriela, Ojala Tiina, Salaets Thomas, Sunnegård Jan, Bhat Misha, Wacker Julie, Wåhlander Håkan, Lubaua Inguna, Herberg Ulrike, Miller Owen, McMahon Colin J
Fondazione CNR-Regione Toscana G. Monasterio (FTGM), National Research Institute (CNR), Pisa, Italy.
Department for Congenital Cardiology and Pediatric Cardiology, University Hospital Schleswig-Holstein, Campus Kiel, Kiel, Germany.
Eur J Pediatr. 2025 May 31;184(6):379. doi: 10.1007/s00431-025-06175-9.
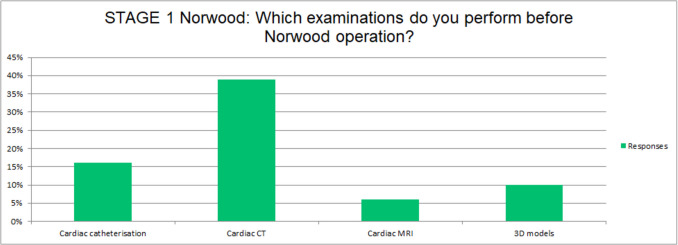
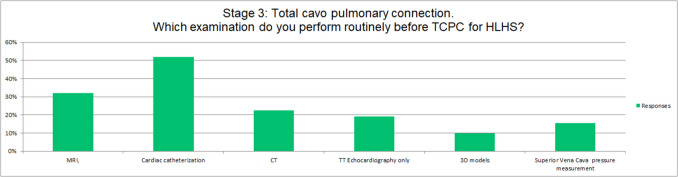
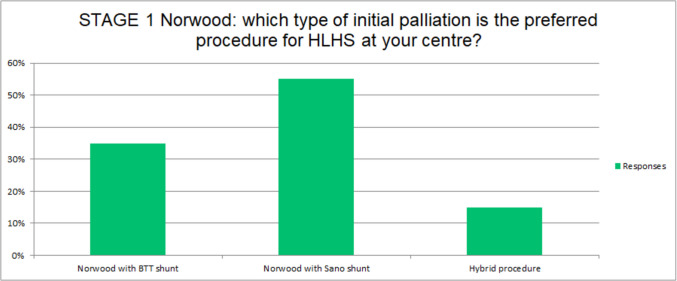
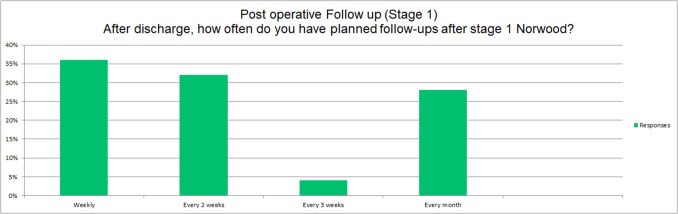
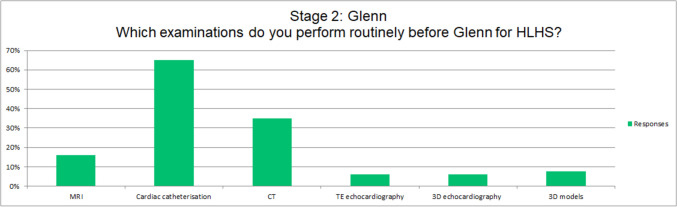
Despite significant advances in knowledge and the development of guidelines, the management of hypoplastic left heart syndrome (HLHS) remains highly variable. A structured questionnaire was circulated across European Association of Paediatric & Congenital Cardiology (AEPC) affiliated centres. The aims were to evaluate standards in pre-operative assessment, types of surgery, follow-up and medical practices in children with HLHS. Thirty-one centres from 20 countries completed the survey. Delivery of babies with HLHS occurred in co-located maternity hospitals in 74% of centres; 29% were planned for spontaneous onset of labour, while 54% decided on a case-by-case basis. The preferred initial palliation was a right ventricle-pulmonary artery conduit in 55% of cases, modified Blalock-Thomas Taussig shunt (mBTTS) in 35%, and hybrid in 15% of cases. Timing for Glenn varied from 3 to 6 months of age and preoperative examination varied greatly: 65% performed cardiac catheterization and only 19% performed cardiac magnetic resonance. Stage III palliation was performed at a highly variable interval (2-6 years of age), nearly always employing an extracardiac conduit. Fenestration was routinely performed in 61% and reserved for borderline cases in 39%. All the centers adopted warfarin for the first 3-12 months after Fontan completion, and continued if a fenestration was present, while in non-fenestrated aspirin was left by most centers (e.g. 68%). However, there was a high disparity in the use of heart failure medications (e.g. in interstage I-II 35% use ACE-inhibitors, and only 26% digoxin). Follow-up practice also varied widely with only 60% employing specific protocols.
This first multi-centre European survey from 31 centres from 20 different European countries highlighted a high practice variation in HLHS management across all the stages of Single Ventricle (Fontan) palliation. Major variations pertained to pre- and post-surgical investigations, surgical strategy for stage I and III, medical treatment regimens, and follow-up programs.
• Hypoplastic left heart syndrome (HLHS) remains one of the most complex and challenging congenital cardiac defects to manage. • Investigating the management of children with HLHS across different European centres can facilitate study of the most effective management strategies.
• Significant variation in HLHS management were reported in relation to pre- and post-surgical examinations, surgical strategy at stage I and III, medical treatment regimens, and follow-up programs. • Greater standardisation of imaging and diagnostic evaluation, medical treatment and follow-up surveillance may improve outcomes for these vulnerable patients and warrants further study.
尽管在知识方面取得了重大进展并制定了指南,但左心发育不全综合征(HLHS)的管理仍存在很大差异。一份结构化问卷在欧洲儿科与先天性心脏病协会(AEPC)附属中心进行了分发。目的是评估HLHS患儿术前评估、手术类型、随访及医疗实践的标准。来自20个国家的31个中心完成了调查。74%的中心在同地的妇产医院分娩HLHS患儿;29%计划自然发动分娩,而54%根据具体情况决定。在55%的病例中,首选的初始姑息治疗是右心室-肺动脉导管,35%是改良布莱洛克-托马斯·陶西格分流术(mBTTS),15%是杂交手术。格林手术的时机从3至6个月龄不等,术前检查差异很大:65%进行心导管检查,只有19%进行心脏磁共振检查。III期姑息治疗在2至6岁的高度可变间隔内进行,几乎总是采用心外导管。61%的病例常规进行开窗,39%的病例留作临界病例。所有中心在Fontan手术完成后的前3至12个月采用华法林,如有开窗则继续使用,而在未开窗的情况下,大多数中心(如68%)使用阿司匹林。然而,在心力衰竭药物的使用上存在很大差异(例如,在I-II期过渡阶段,35%使用血管紧张素转换酶抑制剂,只有26%使用地高辛)。随访实践也差异很大,只有60%采用特定方案。
这项来自20个不同欧洲国家31个中心的首次多中心欧洲调查强调了在单心室(Fontan)姑息治疗的所有阶段,HLHS管理存在很大的实践差异。主要差异涉及术前和术后检查、I期和III期手术策略、药物治疗方案以及随访计划。
• 左心发育不全综合征(HLHS)仍然是最难管理的先天性心脏缺陷之一。• 调查不同欧洲中心HLHS患儿的管理情况有助于研究最有效的管理策略。
• 报告了HLHS管理在术前和术后检查、I期和III期手术策略、药物治疗方案以及随访计划方面存在显著差异。• 成像和诊断评估、药物治疗及随访监测的更大标准化可能改善这些脆弱患者的预后,值得进一步研究。