Fanti Stefano, Robles Barba Javier Jesus, Behr Spencer, Maurer Tobias, Paredes Pilar, Walz Jochen, Duch Joan, Perdigo Marc Simo, Mainta Ismini Charis, Bonnefoy Pierre Benoit, Coulanges Medge, Tang Jun, Seigne Christelle, Wilke Celine, Catafau Ana M, Iagaru Andrei, Aggarwal Rahul
Nuclear Medicine, IRCCS AOU di Bologna, Bologna, Italy;
Nuclear Medicine, Hospital Universitari de Bellvitge, L'Hospitalet de Llobregat, Barcelona, Spain.
J Nucl Med. 2025 Aug 1;66(8):1210-1216. doi: 10.2967/jnumed.124.269266.
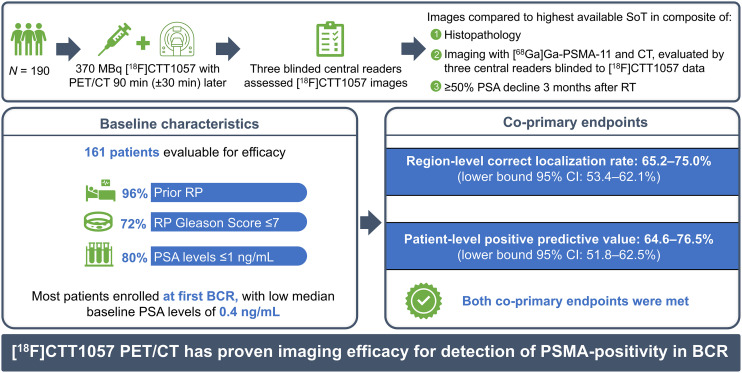
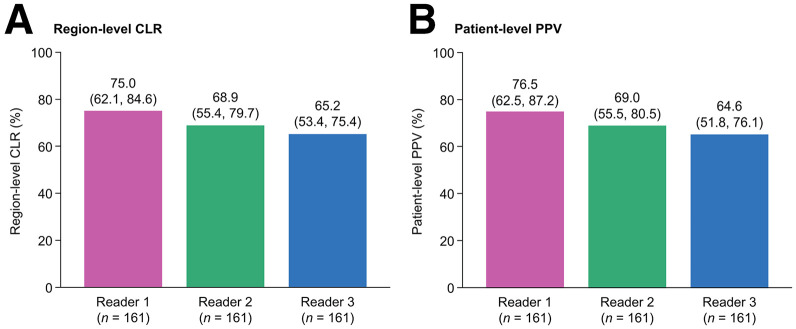
Improved diagnostic accuracy in patients with prostate cancer at first biochemical recurrence (BCR) with low prostate-specific antigen (PSA) levels is needed. This prospective study (GuidePath; NCT04838613) aimed to evaluate the imaging performance of the prostate-specific membrane antigen (PSMA)-targeted PET radiotracer [F]CTT1057 to detect PSMA-positive lesions in patients diagnosed predominantly at first BCR. Eligible patients had a PSA of 0.2 ng/mL or greater after radical prostatectomy or an increase in PSA level of at least 2 ng/mL above nadir after radiation therapy. Patients received 370 MBq of [F]CTT1057 and 150 MBq of [Ga]Ga-PSMA-11 and underwent PET/CT 90 min (±30 min) and 50-100 after injection, respectively. [F]CTT1057 images were assessed by 3 independent readers blinded to all clinical information. Coprimary endpoints were region-level correct localization rate (CLR) and patient-level positive predictive value (PPV) of [F]CTT1057 to detect PSMA-positive lesions and were compared with a hierarchical composite truth standard (CTS). The CTS comprised 3 levels of standard-of-truth procedures (in order of priority): histopathology (CTS level 1); imaging, including at least 1 contrast-enhanced CT scan and 1 [Ga]Ga-PSMA-11 PET/CT scan (CTS level 2); and a decrease in PSA level of 50% or greater 3 mo after radiation therapy (CTS level 3). For study success, the lower-bound 95% CI had to surpass 50% for region-level CLR and 20% for patient-level PPV for at least 2 of the 3 [F]CTT1057 PET/CT readers. Of 202 patients screened, 161 were evaluable for efficacy. Among these, 93.2% were experiencing their first BCR, 96.3% had received radical prostatectomy as initial definitive therapy, and baseline median PSA level was 0.4 ng/mL (interquartile range, 0.3-0.8 ng/mL). The imaging standard of truth was used for 159-160 patients (99%) across the 3 readers. Both coprimary endpoints were met. Region-level CLR ranged from 65.2% to 75.0% (lower-bound 95% CI, 53.4%-62.1%), and patient-level PPV ranged from 64.6% to 76.5% (lower-bound 95% CI, 51.8%-62.5%). [F]CTT1057 met the predefined thresholds for region-level CLR and patient-level PPV in a clinically relevant patient cohort predominantly at first BCR with low PSA levels. [F]CTT1057 is an accurate PSMA-targeted PET radiotracer for BCR detection.
对于首次生化复发(BCR)且前列腺特异性抗原(PSA)水平较低的前列腺癌患者,需要提高诊断准确性。这项前瞻性研究(GuidePath;NCT04838613)旨在评估前列腺特异性膜抗原(PSMA)靶向PET放射性示踪剂[F]CTT1057在主要诊断为首次BCR的患者中检测PSMA阳性病变的成像性能。符合条件的患者在根治性前列腺切除术后PSA为0.2 ng/mL或更高,或在放射治疗后PSA水平比最低点至少升高2 ng/mL。患者接受370 MBq的[F]CTT1057和150 MBq的[Ga]Ga-PSMA-11,并分别在注射后90分钟(±30分钟)和50 - 100分钟接受PET/CT检查。[F]CTT1057图像由3名对所有临床信息不知情的独立阅片者进行评估。共同主要终点是[F]CTT1057检测PSMA阳性病变的区域水平正确定位率(CLR)和患者水平阳性预测值(PPV),并与分层综合真值标准(CTS)进行比较。CTS包括3个真值标准程序级别(按优先级排序):组织病理学(CTS 1级);影像学检查,包括至少1次增强CT扫描和1次[Ga]Ga-PSMA-11 PET/CT扫描(CTS 2级);以及放射治疗后3个月PSA水平下降50%或更多(CTS 3级)。为使研究成功,对于3名[F]CTT1057 PET/CT阅片者中的至少2名,区域水平CLR的下限95%CI必须超过50%,患者水平PPV的下限95%CI必须超过20%。在筛查的202例患者中,161例可进行疗效评估。其中,93.2%为首次BCR,96.3%接受过根治性前列腺切除术作为初始确定性治疗,基线中位PSA水平为0.4 ng/mL(四分位间距,0.3 - 0.8 ng/mL)。在3名阅片者中,159 - 160例患者(99%)采用了影像学真值标准。两个共同主要终点均达到。区域水平CLR范围为65.2%至75.0%(下限95%CI,53.4% - 62.1%),患者水平PPV范围为64.6%至76.5%(下限95%CI,51.8% - 62.5%)。在主要为首次BCR且PSA水平较低的临床相关患者队列中,[F]CTT1057达到了区域水平CLR和患者水平PPV的预定义阈值。[F]CTT1057是一种用于BCR检测的准确的PSMA靶向PET放射性示踪剂。