Söderpalm Bo, Lidö Helga, Franck Johan, Håkansson Anders, Lindqvist Daniel, Heilig Markus, Guterstam Joar, Samuelson Markus, Askerup Barbro, Wallmark-Nilsson Cecilia, de Bejczy Andrea
Addiction Biology Unit, Psychiatry and Neurochemistry Section, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Sweden & Department of Addiction and Dependency, Sahlgrenska University Hospital, Gothenburg, Sweden.
Department of Clinical Neuroscience, Centre for Psychiatry Research, Karolinska Institute & Stockholm Health Care Services, Stockholm County Council, Stockholm, Sweden.
Lancet Reg Health Eur. 2025 May 13;54:101310. doi: 10.1016/j.lanepe.2025.101310. eCollection 2025 Jul.
Alcohol use disorder (AUD) is associated with an enormous burden of disease and cost to society. The dopamine deficiency hypothesis posits that negative reinforcement generated by a low brain dopamine state drives ethanol intake. Here, we evaluated the efficacy and safety of combined administration of two dopamine-enhancing drugs, varenicline (a partial nicotinic acetylcholine receptor agonist) and bupropion (a weak dopamine-reuptake inhibitor) on alcohol intake in AUD.
Participants aged 25-70 years with moderate-to-severe AUD (defined as ≥4/11 Diagnostic and Statistical Manual of Mental Disorders [DSM]-5 criteria) were enrolled in this randomized, double-blind, placebo-controlled trial, done at four outpatient clinics in Sweden. Participants were randomly assigned (block size 8) 1:1:1:1 to Placebo + Placebo, Varenicline + Bupropion, Varenicline + Placebo, or Placebo + Bupropion. After a 1-week titration period, Varenicline was taken as 1 mg orally twice per day and bupropion as 150 mg orally twice per day for 12 weeks. Participants, investigators, and all study personnel were unaware of treatment allocation. The two primary outcomes were phosphatidylethanol in blood (B-PEth) and self-reported percentage heavy drinking days (%HDD), assessed over a steady state 10-week-period (from start of week 2 to end of week 11). Modified intention-to-treat (mITT) and per protocol analyses (PP) were performed using a sequential hierarchical statistical method. This registered study (EudraCT 2018-000048-24; clinicaltrials.govNCT04167306) is completed.
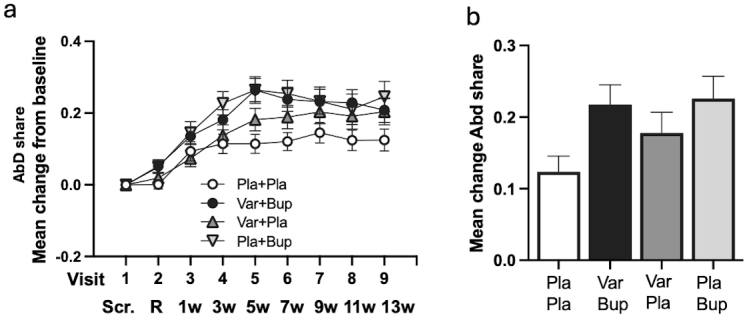
Between March 4, 2019, and December 14, 2022, 384 participants were randomly assigned: Placebo + Placebo = 97, Varenicline + Bupropion = 100, Varenicline + Placebo = 96, Placebo + Bupropion = 91. 72% participants were male (277/384) and 28% female (107/384), median age 57 (13) years. In the mITT analyses, Varenicline + Bupropion reduced B-PEth (Cohen's d [d] = 0·39, p = 0·004) and %HDD (d = 0·31, p = 0·008) vs Placebo + Placebo. Varenicline + Placebo also reduced B-PEth (d = 0·30, p = 0·005) and %HDD (d = 0·36, p = 0·023) vs Placebo + Placebo. For both primary endpoints, differences between the Varenicline + Bupropion and Varenicline + Placebo groups were not statistically significant (B-PEth: d = 0·022, p = 0·97, %HDD: d = 0·027, p = 0·76), precluding further comparisons according to the statistical hierarchy. In PP analyses, both primary outcomes were reduced with Varenicline + Bupropion (d = 0·43 [B-PEth]; d = 0·41 [%HDD]) and Varenicline + Placebo (d = 0·29 [B-PEth]; d = 0·34 [%HDD]) compared with Placebo + Placebo. Nausea, the only safety concern, was more common in the Varenicline + Placebo group than in the Placebo + Placebo group (49/96 vs 11/97, p < 0·0001) and of longer median duration (45 (70) vs 10 (14·5) days, p = 0·001). Nausea incidence was lower in the Varenicline + Bupropion group vs Varenicline + Placebo (36/100 vs 49/96, p = 0·048) and of shorter median duration (16·5 (39·3) vs 45 (70) days, p = 0·010).
Two brain dopamine elevating treatments (Varenicline + Bupropion; Varenicline + Placebo) reduce alcohol consumption compared with placebo alone. Effect sizes were largest when Varenicline and Bupropion were combined and compliance was high (PP-population). Bupropion reduced Varenicline-induced nausea. Varenicline + Bupropion or other mild dopamine enhancers should be further explored for treatment of AUD.
This study was funded primarily by the Swedish Research Council.
酒精使用障碍(AUD)给社会带来了巨大的疾病负担和成本。多巴胺缺乏假说认为,大脑多巴胺水平低下产生的负强化作用驱动了乙醇摄入。在此,我们评估了两种增强多巴胺的药物——伐尼克兰(一种部分烟碱型乙酰胆碱受体激动剂)和安非他酮(一种弱多巴胺再摄取抑制剂)联合使用对AUD患者酒精摄入量的疗效和安全性。
本随机、双盲、安慰剂对照试验在瑞典的四家门诊诊所进行,纳入年龄在25 - 70岁之间、患有中度至重度AUD(定义为≥4/11《精神疾病诊断与统计手册》[DSM]-5标准)的参与者。参与者被随机分配(区组大小为8),按1:1:1:1分为安慰剂 + 安慰剂组、伐尼克兰 + 安非他酮组、伐尼克兰 + 安慰剂组或安慰剂 + 安非他酮组。经过1周的滴定期后,伐尼克兰口服剂量为1 mg,每日两次,安非他酮口服剂量为150 mg,每日两次,持续12周。参与者、研究者和所有研究人员均不知晓治疗分配情况。两个主要结局指标为血液中的磷脂酰乙醇(B - PEth)和自我报告的重度饮酒天数百分比(%HDD),在为期10周的稳定期(从第2周开始至第1周结束)进行评估。采用序贯分层统计方法进行改良意向性分析(mITT)和符合方案分析(PP)。这项注册研究(EudraCT 2018 - 000048 - 24;clinicaltrials.govNCT04167306)已完成。
在2019年3月4日至2022年12月14日期间,384名参与者被随机分配:安慰剂 + 安慰剂组 = 97人,伐尼克兰 + 安非他酮组 = 100人,伐尼克兰 + 安慰剂组 = 96人,安慰剂 + 安非他酮组 = 91人。72%的参与者为男性(277/384),28%为女性(107/384),中位年龄57(13)岁。在mITT分析中,与安慰剂 + 安慰剂组相比,伐尼克兰 + 安非他酮组降低了B - PEth(科恩d值[d] = 0·39,p = 0·004)和%HDD(d = 0·31,p = 0·008)。与安慰剂 + 安慰剂组相比,伐尼克兰 + 安慰剂组也降低了B - PEth(d = 0·30,p = 0·005)和%HDD(d = 0·36,p = 0·023)。对于两个主要终点,伐尼克兰 + 安非他酮组和伐尼克兰 + 安慰剂组之间的差异无统计学意义(B - PEth:d = 0·022,p = 0·97,%HDD:d = 0·027,p = 0·76),因此无法按照统计层次进行进一步比较。在PP分析中,与安慰剂 + 安慰剂组相比,伐尼克兰 + 安非他酮组(针对B - PEth,d = 0·43;针对%HDD,d = 0·41)和伐尼克兰 + 安慰剂组(针对B - PEth,d = 0·29;针对%HDD,d = 0·34)均降低了两个主要结局指标。唯一的安全问题——恶心,在伐尼克兰 + 安慰剂组比在安慰剂 + 安慰剂组更常见(49/96 vs 11/97,p < 0·0001),且中位持续时间更长(45(70)天 vs 10(14·5)天,p = 0·001)。伐尼克兰 + 安非他酮组的恶心发生率低于伐尼克兰 + 安慰剂组(36/100 vs 49/96,p = 0·048),且中位持续时间更短(16·5(39·3)天 vs 45(70)天,p = 0·010)。
与单独使用安慰剂相比,两种提高大脑多巴胺水平的治疗方法(伐尼克兰 + 安非他酮;伐尼克兰 + 安慰剂)可减少酒精消费。当伐尼克兰和安非他酮联合使用且依从性较高时(PP人群),效应量最大。安非他酮减少了伐尼克兰引起的恶心。应进一步探索伐尼克兰 + 安非他酮或其他轻度多巴胺增强剂用于治疗AUD。
本研究主要由瑞典研究理事会资助。