Malakar Sayan, Rungta Sumit, Samanta Arghya, Shamsul Hoda Umair, Mishra Piyush, Pande Gaurav, Roy Akash, Giri Suprabhat, Rai Praveer, Mohindra Samir, Ghoshal Uday C
Department of Gastroenterology, King George's Medical University, Lucknow 226003, Uttar Pradesh, India.
Department of Medical Gastroenterology, King George's Medical University, Lucknow 226003, Uttar Pradesh, India.
World J Hepatol. 2025 May 27;17(5):104724. doi: 10.4254/wjh.v17.i5.104724.
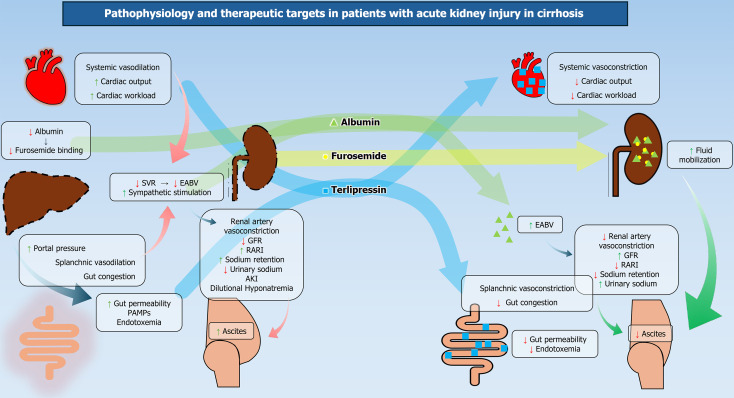
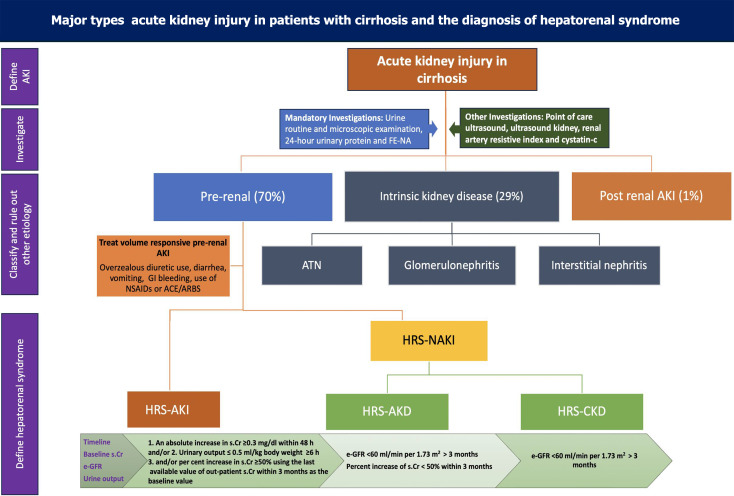
Acute kidney injury (AKI) is present in 30%-40% of hospitalized patients with cirrhosis. Its incidence is higher in patients with severe alcoholic hepatitis, spontaneous bacterial peritonitis, and acute-on-chronic-liver failure (ACLF). Kidney injury is an important landmark event in the natural history of cirrhosis as it is associated with higher mortality. Overwhelming systemic vasodilation, cardiac dysfunction, hypoperfusion, endotoxemia, and direct nephrotoxicity predispose patients with cirrhosis to kidney injury. Infection is present in 25% of patients with decompensated cirrhosis and 35%-40% of patients with ACLF. Advanced cirrhosis with portal hypertension leads to a sluggish portal flow, leading to increased gut congestion, altered gut permeability and bacterial translocations. They drive infection and endotoxemia in such patients. Pathogen-associated molecular patterns activate inflammatory cascades, which leads to further deterioration in hemodynamics and reduced glomerular filtration rate. Infections and pro-inflammatory cytokines like interleukin 6 (IL-6), IL-1, and tumor necrosis factor alpha may directly cause kidney parenchymal injury. The combined effect of dysfunctional albumin and systemic and splanchnic vasodilatation leads to low effective blood volume, activating the renin-angiotensin-aldosterone system. This causes renal vasoconstriction, water retention, and ascites, which progresses to hepatorenal physiology and AKI development. Vasoconstriction and volume expansion effectively improve arterial blood volume and systemic hemodynamics, thereby improving renal blood flow. It is of paramount importance to predict, detect, and treat AKI in its early state, as progressive renal dysfunction is invariably associated with higher mortality in patients with decompensated cirrhosis and ACLF. This comprehensive review will focus on the recent evolving concepts of the pathophysiology, diagnosis, and management of AKI in patients with cirrhosis.
30%-40%的肝硬化住院患者存在急性肾损伤(AKI)。在重症酒精性肝炎、自发性细菌性腹膜炎和慢加急性肝衰竭(ACLF)患者中,其发病率更高。肾损伤是肝硬化自然病程中的一个重要标志性事件,因为它与更高的死亡率相关。全身性血管扩张、心脏功能障碍、灌注不足、内毒素血症和直接肾毒性使肝硬化患者易发生肾损伤。25%的失代偿期肝硬化患者和35%-40%的ACLF患者存在感染。伴有门静脉高压的晚期肝硬化导致门静脉血流缓慢,进而导致肠道淤血增加、肠道通透性改变和细菌易位。它们促使此类患者发生感染和内毒素血症。病原体相关分子模式激活炎症级联反应,导致血流动力学进一步恶化和肾小球滤过率降低。感染以及白细胞介素6(IL-6)、IL-1和肿瘤坏死因子α等促炎细胞因子可能直接导致肾实质损伤。功能失调的白蛋白以及全身和内脏血管扩张的综合作用导致有效血容量降低,激活肾素-血管紧张素-醛固酮系统。这会导致肾血管收缩、水潴留和腹水,进而发展为肝肾综合征和AKI。血管收缩和容量扩张可有效改善动脉血容量和全身血流动力学,从而改善肾血流量。在早期预测、检测和治疗AKI至关重要,因为在失代偿期肝硬化和ACLF患者中,进行性肾功能障碍总是与更高的死亡率相关。本综述将聚焦于肝硬化患者AKI病理生理学、诊断和管理方面的最新进展。