Guan Shasha, Ye Qianwen, Li Panhua, Ding Lijuan
Oncology Department, Hainan Hospital of Chinese People's Liberation Army (PLA) General Hospital, Sanya, China.
Front Oncol. 2025 Jun 12;15:1581927. doi: 10.3389/fonc.2025.1581927. eCollection 2025.
Thyroid metastasis is a relatively uncommon event in clinical practice, typically occurs in more prevalent primary tumors, including renal cell carcinoma and cancers of the gastrointestinal tract, lungs, and breast. The incidence of thyroid metastasis from primary hepatocellular carcinoma (HCC) is particularly infrequent. This case report outlines the clinical challenges and diagnostic pathway associated with a thyroid mass in a patient with HCC, highlighting the rarity and intricacy of such metastatic associations.
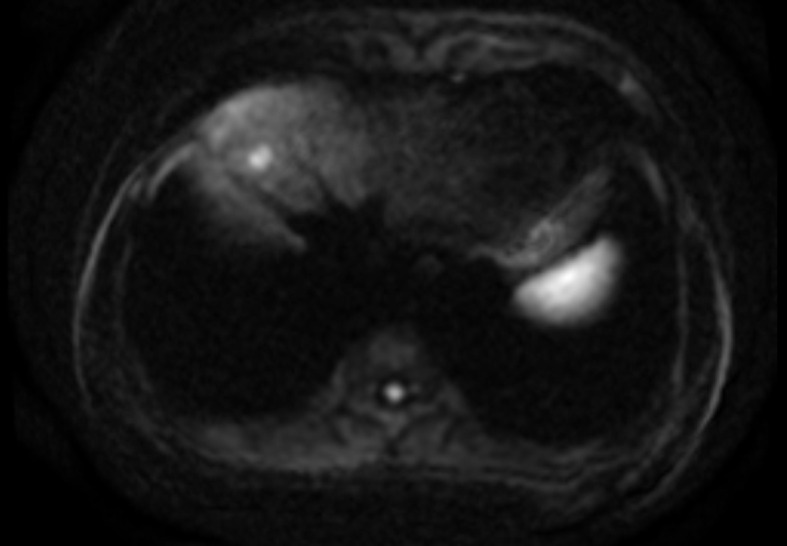
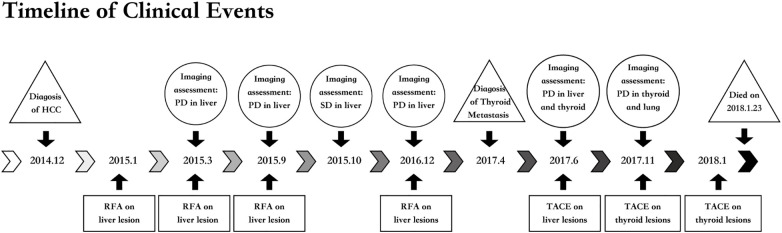
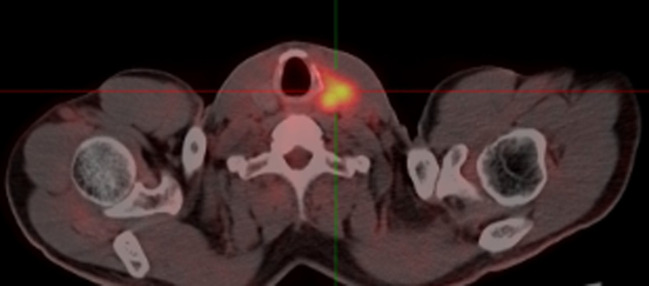
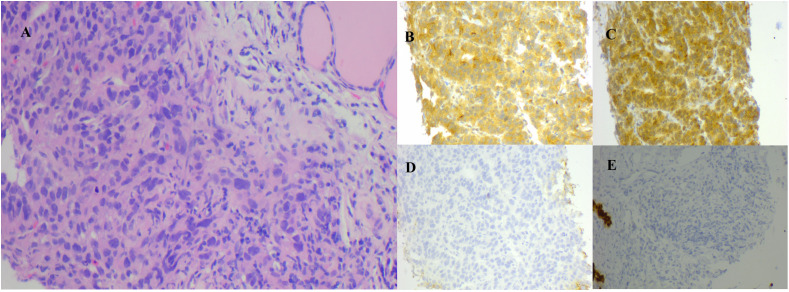
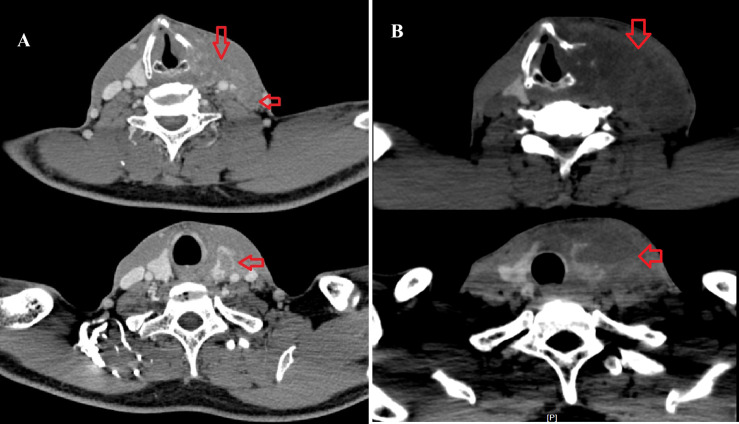
A 51-year-old male with a long-standing history of hepatitis B-related liver cirrhosis presented with a rapidly enlarging painful left-sided thyroid mass 28 months after a diagnosis of HCC. FDG-PET/CT imaging revealed a 6 cm hypodense tumor in the left lobe of the thyroid and further fine needle aspiration cytology and biopsy (FNAB) confirmed it as a metastasis from HCC. The patient underwent transcatheter arterial chemotherapy embolization (TACE) as a first attempt to control the progress of the thyroid lesion. However, subsequent imaging showed a continued progression of the lesions in liver, along with other metastatic sites. Although multiple interventions, such as radiofrequency ablation (RFA) procedures was administered due to the progression of liver cancer and embolization therapies for the thyroid, the patient experienced significant deterioration, presenting with respiratory failure due to malignant pleural effusion.
This unique case highlights the importance of promptly considering persistent or newly developed thyroid nodules as indicative of metastatic disease. The identification of thyroid metastases, especially in the context of extensive organ involvement, often correlates with a poor prognosis. Given the distinctive physiological properties of the thyroid gland, multidisciplinary management may offer clinical benefits for such patients with complex metastatic profiles. Combining locoregional therapies with immunotherapy, particularly dual immunotherapy, may offer significant prognostic advantages. Nevertheless, these hypotheses need to be verified through large-scale clinical trials.
甲状腺转移在临床实践中相对少见,通常发生于更常见的原发性肿瘤,包括肾细胞癌以及胃肠道、肺和乳腺的癌症。原发性肝细胞癌(HCC)转移至甲状腺的发生率尤其低。本病例报告概述了一名HCC患者甲状腺肿物相关的临床挑战和诊断途径,突出了这种转移关联的罕见性和复杂性。
一名有长期乙型肝炎相关性肝硬化病史的51岁男性,在诊断为HCC 28个月后出现左侧甲状腺肿物迅速增大且伴有疼痛。氟代脱氧葡萄糖正电子发射断层扫描/计算机断层扫描(FDG-PET/CT)成像显示甲状腺左叶有一个6厘米的低密度肿瘤,进一步的细针穿刺细胞学检查和活检(FNAB)证实为HCC转移。患者首先接受了经导管动脉化疗栓塞术(TACE)以控制甲状腺病变的进展。然而,后续成像显示肝脏及其他转移部位的病变持续进展。尽管由于肝癌进展对肝脏进行了多次干预,如射频消融(RFA)手术,并对甲状腺进行了栓塞治疗,但患者病情仍显著恶化,因恶性胸腔积液出现呼吸衰竭。
这个独特的病例强调了及时将持续存在或新出现的甲状腺结节视为转移性疾病的重要性。甲状腺转移的识别,尤其是在广泛器官受累的情况下,往往与预后不良相关。鉴于甲状腺独特的生理特性,多学科管理可能为此类具有复杂转移情况的患者带来临床益处。将局部区域治疗与免疫治疗,特别是双重免疫治疗相结合,可能具有显著的预后优势。然而,这些假设需要通过大规模临床试验来验证。