Zhang Xinxing, Wang Yuxuan
Chengdu New Radiomedicine Technology Co. Ltd., Chengdu, Sichuan, China.
Department of Nephrology, Chengdu Second People's Hospital, Chengdu, Sichuan, China.
PLoS One. 2025 Jun 27;20(6):e0326429. doi: 10.1371/journal.pone.0326429. eCollection 2025.
The role of radical prostatectomy (RP) in patients with newly diagnosed bone-metastatic prostate cancer (PCa) remains insufficiently explored.
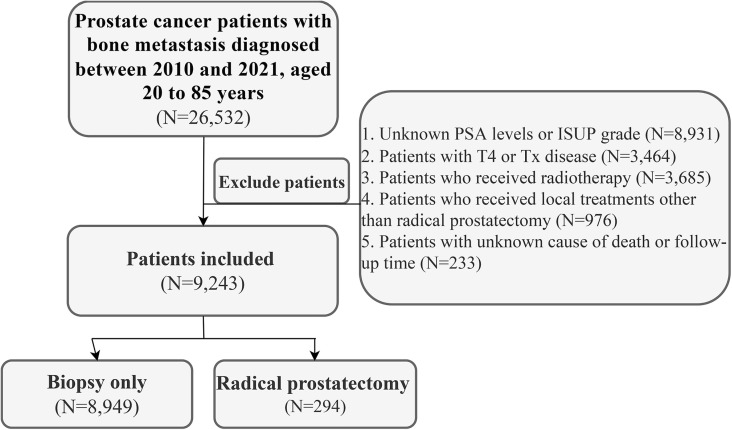
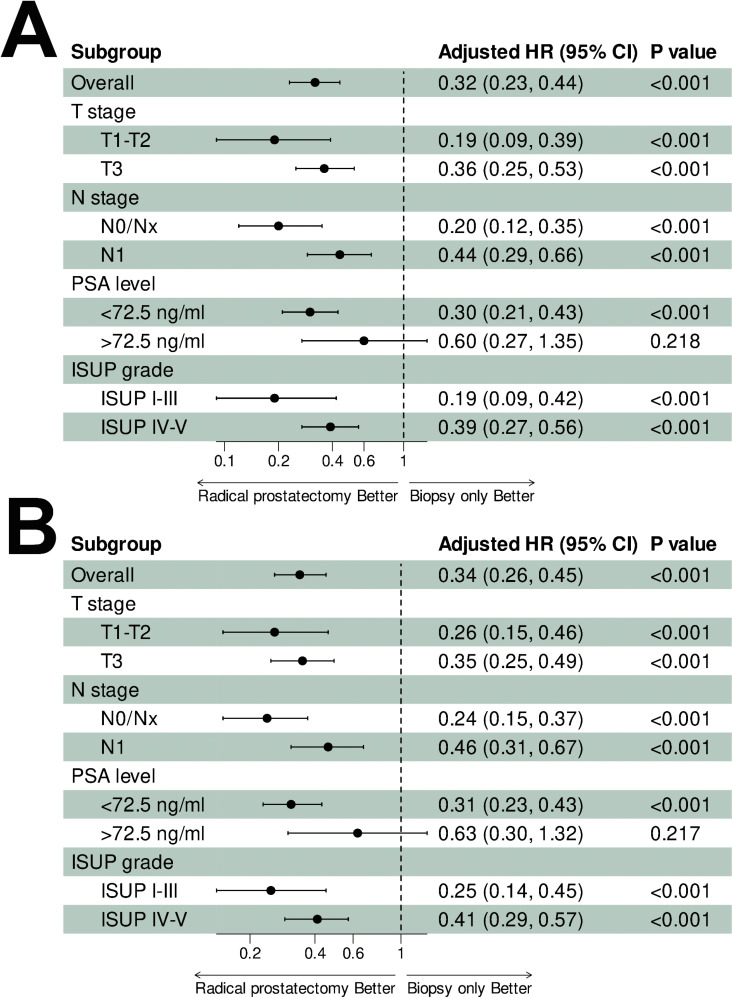
Patients with newly diagnosed bone-metastatic PCa were retrospectively identified from the SEER-17 database and categorized into two groups based on local treatment: biopsy-only and RP. Notably, patients who had received radiotherapy were excluded due to the unavailability of radiotherapy target site details in the SEER database, which made it impossible to determine whether the radiotherapy was directed at metastatic lesions or the prostate. Kaplan-Meier methods were used to estimate cancer-specific survival (CSS) and overall survival (OS) between the two groups. Subgroup analyses stratified by T stage, N stage, PSA levels, and ISUP grade were conducted to assess the impact of disease characteristics on the efficacy of RP. A risk score incorporating these disease characteristics (T stage, N stage, PSA level, ISUP grade) was assigned to each patient, and risk-stratified subgroup analyses were performed to further evaluate the relationship between the efficacy of RP and overall disease characteristics.
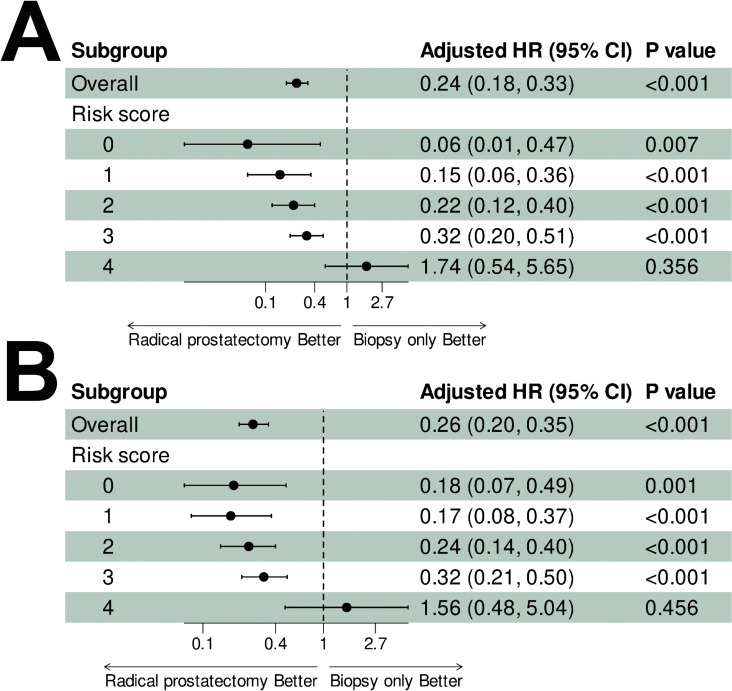
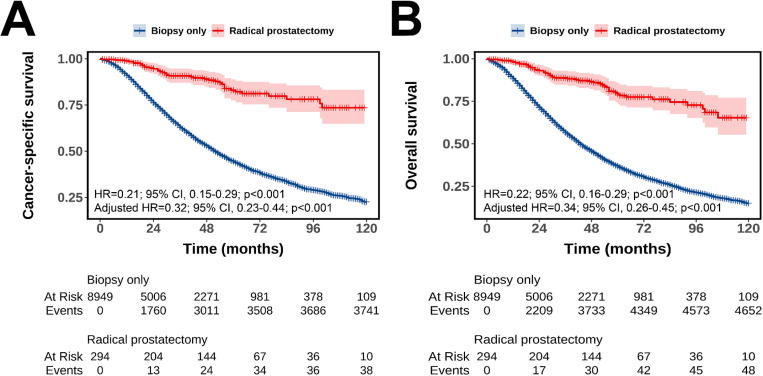
A total of 9,243 patients were included in this study, of whom 8,949 (96.8%) underwent biopsy alone and 294 (3.2%) underwent RP. Patients who underwent RP had better CSS (adjusted HR = 0.32, 95% CI: 0.23-0.44, p < 0.001; 5-year CSS rate: 83.0% vs. 44.5%) and OS (adjusted HR = 0.34, 95% CI: 0.26-0.45, p < 0.001; 5-year OS rate: 79.2% vs. 36.9%) compared with patients who underwent biopsy alone. The survival benefit persisted across all subgroups but were attenuated in patients with more advanced stage (T3 and N1) and higher grades of disease (PSA > 72.5 ng/ml and ISUP grade IV-V). Risk score analysis revealed diminishing benefits with increasing scores. Significant survival benefits were observed for scores 0-3 (all adjusted HR < 1, p < 0.05), whereas no survival differences were detected at the highest risk score (CSS: adjusted HR = 1.74, 95% CI: 0.54-5.65, p = 0.356; OS: adjusted HR = 1.56, 95% CI: 0.48-5.04, p = 0.456).
Survival benefits of RP in de novo bone metastatic prostate cancer are modulated by disease characteristics, with attenuated effects in advanced/high-grade disease. Risk-stratified patient selection is critical, and prospective studies are needed to validate optimal candidacy for RP.
根治性前列腺切除术(RP)在新诊断的骨转移前列腺癌(PCa)患者中的作用仍未得到充分探索。
从SEER - 17数据库中回顾性识别出新诊断的骨转移PCa患者,并根据局部治疗方式分为两组:仅活检组和RP组。值得注意的是,由于SEER数据库中没有放疗靶区详细信息,接受过放疗的患者被排除在外,这使得无法确定放疗是针对转移灶还是前列腺。采用Kaplan - Meier方法估计两组之间的癌症特异性生存(CSS)和总生存(OS)。进行按T分期、N分期、PSA水平和ISUP分级分层的亚组分析,以评估疾病特征对RP疗效的影响。为每位患者分配一个包含这些疾病特征(T分期、N分期、PSA水平、ISUP分级)的风险评分,并进行风险分层亚组分析,以进一步评估RP疗效与整体疾病特征之间的关系。
本研究共纳入9243例患者,其中8949例(96.8%)仅接受活检,294例(3.2%)接受RP。与仅接受活检的患者相比,接受RP的患者具有更好的CSS(调整后HR = 0.32,95%CI:0.23 - 0.44,p < 0.001;5年CSS率:83.0%对44.5%)和OS(调整后HR = 0.34,95%CI:0.26 - 0.45,p < 0.001;5年OS率:79.2%对36.9%)。生存获益在所有亚组中均持续存在,但在更晚期(T3和N1)和更高疾病分级(PSA > 72.5 ng/ml和ISUP分级IV - V)的患者中有所减弱。风险评分分析显示,随着评分增加,获益逐渐减少。在评分0 - 3时观察到显著的生存获益(所有调整后HR < 1,p < 0.05),而在最高风险评分时未检测到生存差异(CSS:调整后HR = 1.74,95%CI:0.54 - 5.65,p = 0.356;OS:调整后HR = 1.56,95%CI:0.48 - 5.04,p = 0.456)。
RP在新发骨转移前列腺癌中的生存获益受疾病特征调节,在晚期/高分级疾病中作用减弱。风险分层的患者选择至关重要,需要前瞻性研究来验证RP的最佳候选资格。