Tran Henri, Caruso Stefano, Mazialivoua Anne-Laure, Fargeat Cecile, Rousselet Odile, Ko Adrien, Leroy Vincent, Ingiliz Patrick
Hepatology Department, Henri-Mondor University Hospital, Inserm Unit 955, 1, rue Gustave Eiffel, Créteil, 94000, France.
Cerba Healthcare, Saint-Ouen-l'Aumône, France.
BMC Gastroenterol. 2025 Jul 1;25(1):454. doi: 10.1186/s12876-025-03992-y.
The ideal non-invasive marker to identify patient at risk for liver fibrosis in the general population is unknown. Current guidelines (EASL) recommend using the FIB-4 score as a screening tool but the low specificity may result in a large number of potentially false-positive results. Recently, the liver risk score (LRS) has been suggested to more accurately identify patients at-risk. The aim of our study was to identify populations at-risk using the two scores.
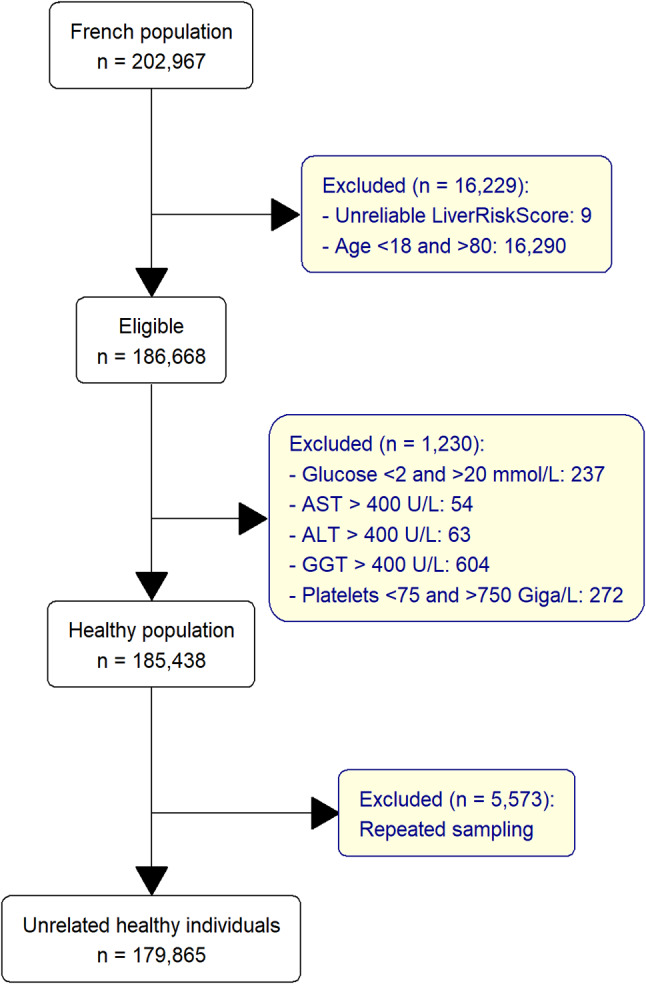
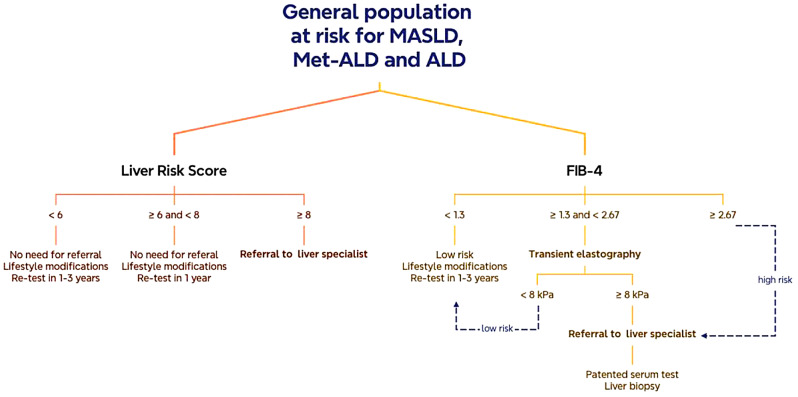
“Cerbafib” was a prospective cohort derived from laboratories throughout the Paris region. The prevalence of advanced liver fibrosis was assessed using the non-invasive FIB-4 score with a cut-off of 2.67 (rule-in) and 1.3 (rule-out) and the LRS with a cut-off of < 6 (minimal risk), ≥ 6 to < 10 (low risk), ≥ 10 to < 15 (medium risk) and ≥ 15 (high risk).
Between January and April 2023, 179 865 patients were included in the cohort. The mean age was 52 years and 45% were men. FIB-4 identified 55 376 (31%) patients requiring specialist referral ( ≥ = 1.3) and 4002 patients (2.2%) with suspected advanced fibrosis. LRS identified 38 175 (21%) patients with estimated liver stiffness ≥ 6 kPa, 1 933 patients (1%) ≥ 10 kPa and 35 (0.02%) patients ≥ 15 kPa. There was a poor correlation between the two tests ( = 0.45).
The Liver Risk Score is a practical tool to identify a population in need of further hepatologic evaluation. Compared to FIB-4, the population identified by LRS is smaller and different. An adapted new pragmatic screening algorithm using LRS should be considered.
在普通人群中,用于识别有肝纤维化风险患者的理想非侵入性标志物尚不清楚。当前指南(欧洲肝脏研究学会)推荐使用FIB-4评分作为筛查工具,但低特异性可能导致大量潜在的假阳性结果。最近,有人提出肝脏风险评分(LRS)能更准确地识别有风险的患者。我们研究的目的是使用这两种评分来识别有风险的人群。
“Cerbafib”是一个来自巴黎地区各实验室的前瞻性队列。使用非侵入性FIB-4评分(截断值为2.67(纳入标准)和1.3(排除标准))以及肝脏风险评分(截断值为<6(最低风险)、≥6至<10(低风险)、≥10至<15(中度风险)和≥15(高风险))评估晚期肝纤维化的患病率。
在2023年1月至4月期间,该队列纳入了179865名患者。平均年龄为52岁,45%为男性。FIB-4识别出55376名(31%)需要专科转诊的患者(≥=1.3)以及4002名(2.2%)疑似晚期纤维化的患者。肝脏风险评分识别出38175名(21%)估计肝脏硬度≥6kPa的患者、1933名(1%)≥10kPa的患者和35名(0.02%)≥15kPa的患者。两种检测之间的相关性较差(=0.45)。
肝脏风险评分是识别需要进一步肝脏学评估人群的实用工具。与FIB-4相比,肝脏风险评分识别出的人群规模更小且有所不同。应考虑采用一种采用肝脏风险评分的适应性新实用筛查算法。