Gittus Matthew, O'Cathain Alicia, Miller Katherine, Oklopcic Anja, Ong Albert C, Fotheringham James
University of Sheffield, Sheffield, UK.
Sheffield Kidney Institute, Northern General Hospital, Sheffield, UK.
BMC Med. 2025 Jul 1;23(1):364. doi: 10.1186/s12916-025-04194-9.
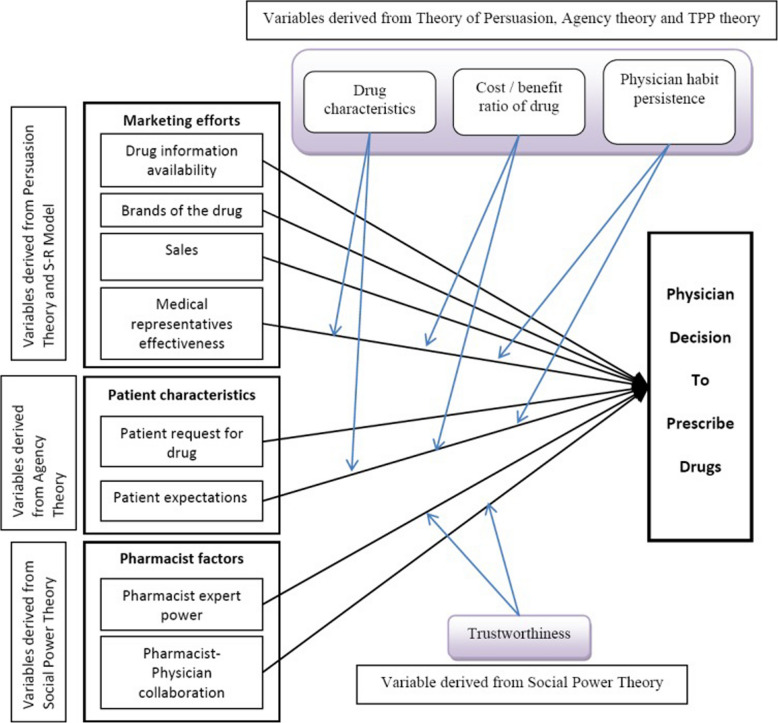
Nearly half of all adults are affected by chronic conditions with long-term medications often being the primary intervention. Although models like that of Murshid and Mohaidin contribute to our understanding of prescribing behaviours, they are not specific to chronic conditions and may not reflect the full range of influencing factors relevant to long-term care. Better understanding the factors that may influence healthcare professionals' decision-making could help inform policy and guidelines as well as identify targets for future research and interventions.
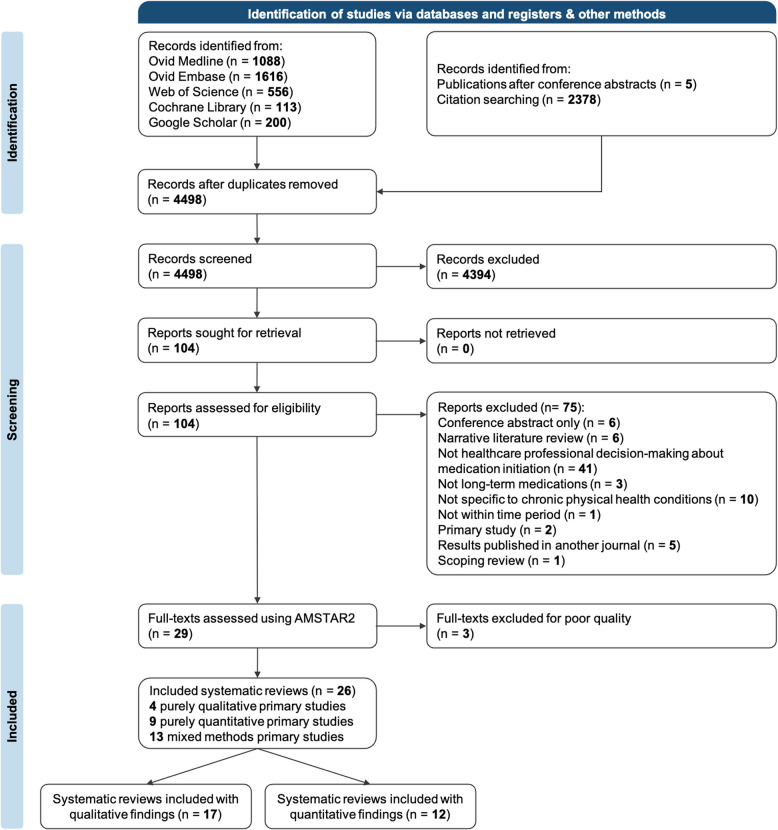
An overview of systematic reviews was undertaken, following the 2020 PRISMA guidelines. PubMed, Embase, Web of Science, Cochrane Library and Google Scholar were searched from 01/01/2013 to 7/11/2023. Quality assessment was undertaken using the AMSTAR 2 tool. Screening, data extraction and synthesis were conducted. Confidence in findings was assessed using the GRADE-CERQual tool. An existing generic conceptual model of prescribing was adjusted to specifically reflect chronic conditions.
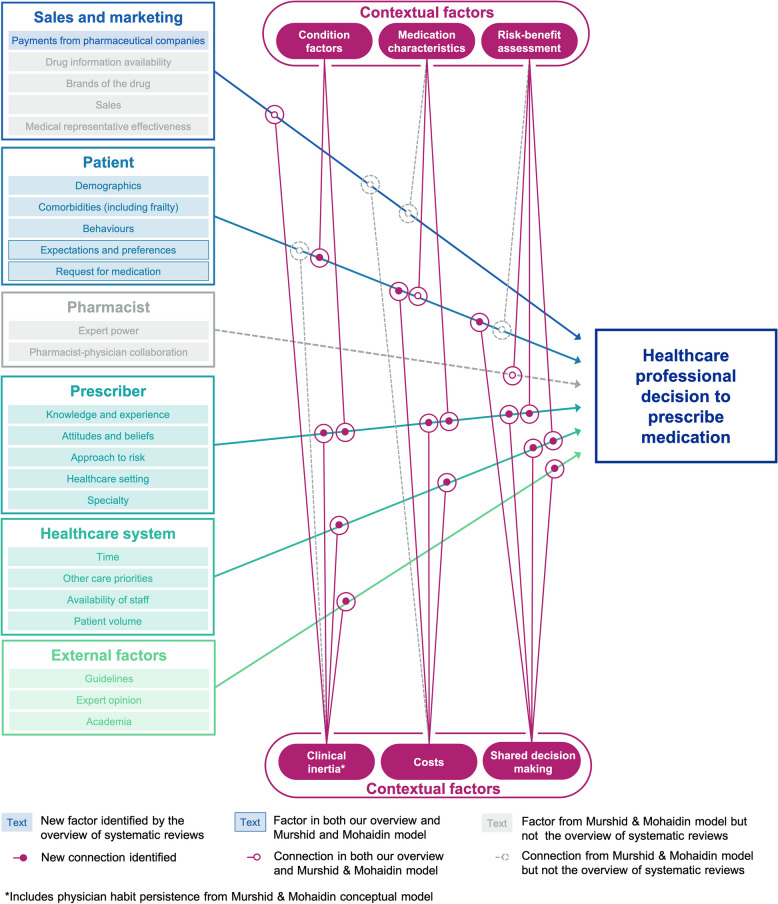
Twenty-six reviews published between 2013 and 2023 were included, synthesising 689 primary studies. Patient factors that may influence prescribers' decisions included age, ethnicity, education and level of rurality of residence. Prescribers describe assessing individual patient characteristics when weighing the risks and benefits, with a tendency to prioritise risks-especially for patients with multiple comorbidities or complex needs. Prescribers' approach to risk may be influenced by their clinical experience, care setting and assessment tools. High workload and competing priorities may lead to clinical inertia in terms of delaying or preventing medication initiation. Shared decision-making may not always be shared equally between patients and prescribers. Beyond direct medication costs, prescribers may also consider broader healthcare costs, such as the need for monitoring and use of support staff for monitoring. External factors such as guidelines may be helpful in navigating risks, with their effectiveness potentially enhanced when they offer specific recommendations tailored to prescribers' population characteristics.
Prescribers may need to navigate multiple challenges when making prescribing decisions for people with chronic conditions. This overview of systematic reviews suggests possible interrelated factor categories influencing prescribing decisions. The conceptual model may be used as a framework for future research and development of interventions.
近一半的成年人受慢性病影响,长期药物治疗通常是主要干预措施。尽管像穆尔希德和莫海丁的模型有助于我们理解处方行为,但它们并非专门针对慢性病,可能无法反映与长期护理相关的所有影响因素。更好地理解可能影响医疗保健专业人员决策的因素,有助于为政策和指南提供信息,并确定未来研究和干预的目标。
按照2020年PRISMA指南进行系统评价概述。在2013年1月1日至2023年11月7日期间检索了PubMed、Embase、科学网、考克兰图书馆和谷歌学术。使用AMSTAR 2工具进行质量评估。进行筛选、数据提取和综合分析。使用GRADE-CERQual工具评估对研究结果的信心。对现有的通用处方概念模型进行调整,以专门反映慢性病情况。
纳入了2013年至2023年发表的26篇综述,综合了689项原始研究。可能影响开处方者决策的患者因素包括年龄、种族、教育程度和居住地区的农村程度。开处方者在权衡风险和益处时会描述评估个体患者特征,倾向于优先考虑风险——尤其是对于患有多种合并症或有复杂需求的患者。开处方者对风险的处理方式可能受其临床经验、护理环境和评估工具的影响。高工作量和相互竞争的优先事项可能导致在延迟或阻止开始用药方面出现临床惰性。共同决策在患者和开处方者之间可能并不总是平等分享。除了直接的药物成本外,开处方者还可能考虑更广泛的医疗保健成本,例如监测需求以及使用辅助人员进行监测的情况。指南等外部因素可能有助于应对风险,当它们针对开处方者的人群特征提供具体建议时,其有效性可能会增强。
开处方者在为慢性病患者做出处方决策时可能需要应对多重挑战。这一系统评价概述表明了可能影响处方决策的相互关联的因素类别。该概念模型可作为未来研究和干预措施开发的框架。