Qiao Lingya, Lin Ying, Liu Mengyang, Liu Jiaqi, Li Ke, Chen Juan, Shi Qiang
Department of Neurology, Tianjin Huanhu Hospital, Tianjin, China.
Department of Neurology, The First Medical Center of Chinese PLA General Hospital, Beijing, China.
Front Immunol. 2025 Jun 17;16:1608735. doi: 10.3389/fimmu.2025.1608735. eCollection 2025.
This study aimed to examine the clinical and muscle histological characteristics of anti-Ku-positive patients. A preliminary investigation into the involvement of autophagy was conducted as well.
Clinical characteristics, laboratory findings, and muscle histological features were collected from patients with isolated anti-Ku antibodies at the Department of Neurology, First Medical Center of the PLA General Hospital, between February 2011 to June 2024. Autophagy-related protein levels were semi-quantitatively assessed on muscle tissue samples using western blot (WB), with sporadic inclusion body myositis (sIBM) and immune-mediated necrotizing myopathy (IMNM) patients as comparison groups.
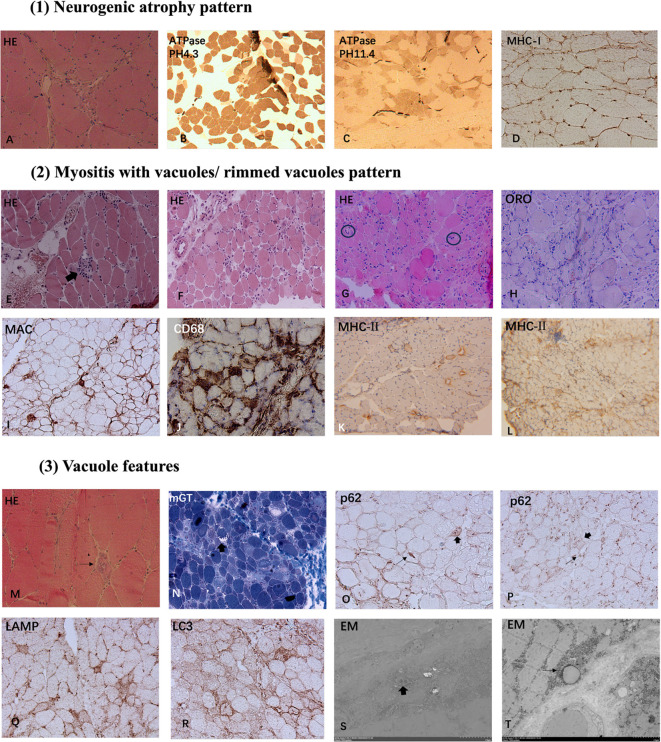
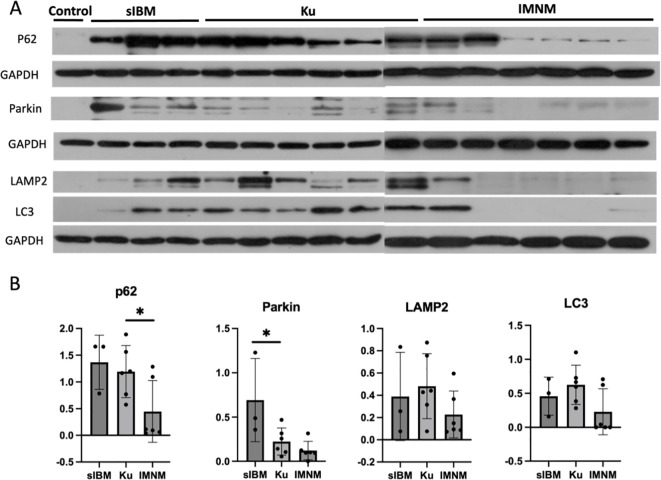
A total of 6 patients were recruited in the study (50% female, mean age at onset 47.6 ± 15.56 years, mean disease duration 7 ± 5.58 months). Extramuscular involvement was observed in most cases, including subcutaneous edema (33.3%), skin rash (33.3%), hyperpigmentation (33.3%), hair loss (33.3%), arthralgia (50%), and interstitial lung disease (ILD) (33.3%), etc. Coexisting connective tissue diseases included systemic sclerosis (SSc) (83.3%), systemic lupus erythematosus (SLE) (16.7%), and arthritis (16.7%). The distribution of muscle weakness was generally symmetrical and proximal (83.3%). Distal (50%) and axial (50%) muscle weakness could also be found. 2 patients exhibited peripheral nerve damage and myogenic damage in EMG, while 4 showed myogenic damage. Creatine kinase (CK) was mildly or moderately elevated. Muscle biopsy demonstrated two patterns: a neurogenic atrophy pattern and a myositis pattern characterized by a varying degree of necrotizing fibers (100%) with rimmed vacuoles (50%) or non-rimmed vacuoles (50%). Immunohistochemical (IHC) analysis revealed sarcolemma deposition of major histocompatibility complex class I (MHC-I) (83.3%) and MHC-II (83.3%), as well as predominant CD68-positive inflammatory infiltrates (66.7%). IHC for p62 revealed a sarcoplasmic punctate pattern (50%), along with a focal coarse staining pattern (50%) and occasional fine granular staining (33.3%). Electron microscopy (EM) demonstrated filamentous and lipid accumulation within vacuoles. WB analysis showed that p62 levels significantly differed between the anti-Ku and IMNM groups. Additionally, Parkin levels were highest in sIBM, while lysosome-associated membrane protein 2 (LAMP2) and microtubule-associated protein 1A/1B-light chain 3 (LC3) expression was highest in the anti-Ku-positive group in tendency.
The muscular features were heterogeneous in anti-Ku-positive patients. A predominant myositis pattern was characterized by necrotizing fibers and vacuolar changes in muscle histology, which differ from sIBM and IMNM. Autophagy appeared to be a key mechanism implicated in the pathogenesis.
本研究旨在探讨抗Ku抗体阳性患者的临床及肌肉组织学特征,并初步研究自噬在其中的作用。
收集2011年2月至2024年6月期间解放军总医院第一医学中心神经内科孤立性抗Ku抗体患者的临床特征、实验室检查结果及肌肉组织学特征。采用蛋白质免疫印迹法(WB)对肌肉组织样本中自噬相关蛋白水平进行半定量评估,以散发性包涵体肌炎(sIBM)和免疫介导坏死性肌病(IMNM)患者作为对照组。
本研究共纳入6例患者(50%为女性,平均发病年龄47.6±15.56岁,平均病程7±5.58个月)。多数患者存在肌外表现,包括皮下水肿(33.3%)、皮疹(33.3%)、色素沉着(33.3%)、脱发(33.3%)、关节痛(50%)和间质性肺疾病(ILD)(33.3%)等。并存的结缔组织病包括系统性硬化症(SSc)(83.3%)、系统性红斑狼疮(SLE)(16.7%)和关节炎(16.7%)。肌无力分布多为对称性近端受累(83.3%),也可见远端(50%)和躯干部(50%)肌无力。2例患者肌电图显示周围神经损害和肌源性损害,4例显示肌源性损害。肌酸激酶(CK)轻度或中度升高。肌肉活检显示两种模式:神经源性萎缩模式和肌炎模式,其特征为不同程度的坏死纤维(100%),伴有镶边空泡(50%)或非镶边空泡(50%)。免疫组织化学(IHC)分析显示主要组织相容性复合体I类(MHC-I)(83.3%)和MHC-II(83.3%)在肌膜沉积,以及主要为CD68阳性的炎性浸润(66.7%)。p62免疫组化显示肌浆点状模式(50%),伴有局灶性粗染色模式(50%)和偶尔的细颗粒状染色(33.3%)。电子显微镜(EM)显示空泡内有丝状和脂质积聚。WB分析显示抗Ku组和IMNM组之间p62水平有显著差异。此外,Parkin水平在sIBM中最高,而溶酶体相关膜蛋白2(LAMP2)和微管相关蛋白1A/1B轻链3(LC3)表达在抗Ku抗体阳性组中呈升高趋势。
抗Ku抗体阳性患者的肌肉特征具有异质性。主要的肌炎模式在肌肉组织学上表现为坏死纤维和空泡改变,这与sIBM和IMNM不同。自噬似乎是发病机制中的关键机制。