Einarsdottir Sigrun, Lobaugh Stephanie, Luan Danny, Gomez-Llobell Marina, Subramanian Padmapriya, Devlin Sean, Chung David, Dahi Parastoo B, Falchi Lorenzo, Giralt Sergio, Landau Heather, Lesokhin Alexander M, Lin Richard, Lue Jennifer, Mailankody Sham, Palomba M Lia, Park Jae H, Salles Gilles, Scordo Michael, Escribano-Serrat Silvia, Sanz Jaime, Rejeski Kai, Shouval Roni, Usmani Saad, Perales Miguel-Angel, Shah Gunjan, Shahid Zainab
Adult Bone Marrow Transplant Service, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Department of Hematology, Sahlgrenska University Hospital, Gothenburg, Sweden.
Blood Cancer J. 2025 Jul 2;15(1):114. doi: 10.1038/s41408-025-01321-w.
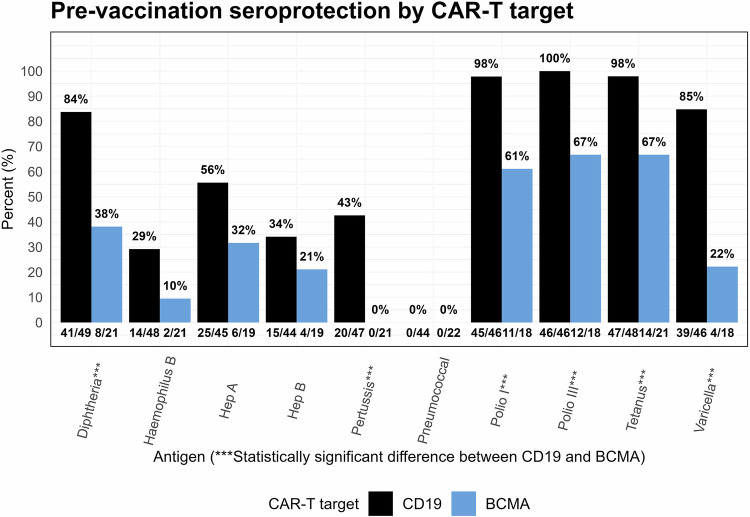
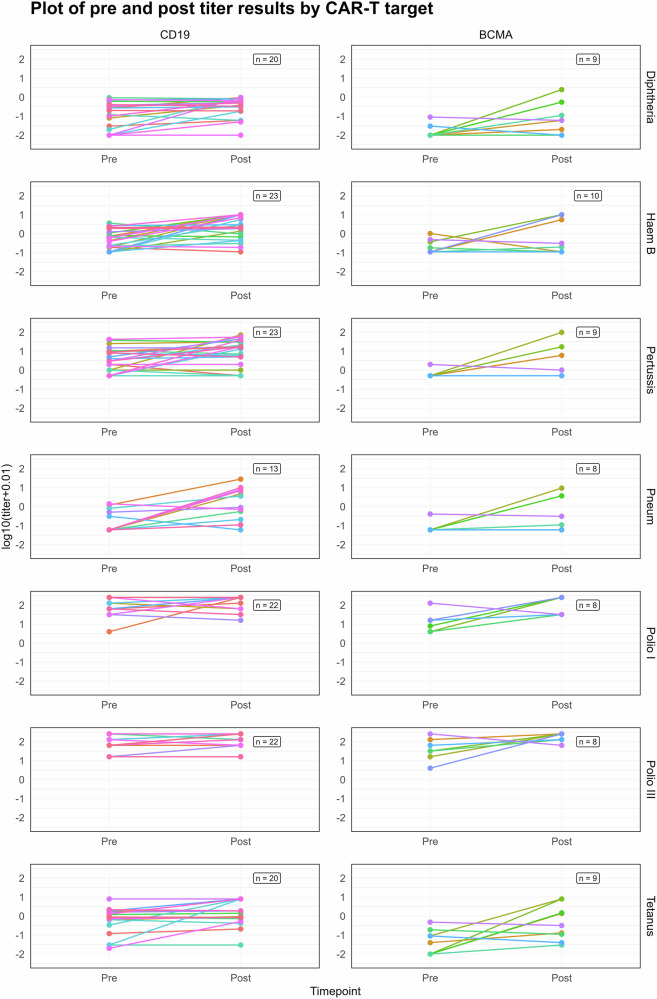
This single-center, retrospective study analyzed vaccine responses in patients who received post-Chimeric Antigen Receptor (CAR) T-cell therapy vaccination between 2018 and 2024. Vaccinations were administered according to EBMT/CIBMTR recommendations and pathogen-specific IgG responses to 12 vaccine-preventable infections were assessed. Seroprotection was defined by established cut-offs or a significant fold increase in titers. A total of 73 patients that had not received intravenous immunoglobulins within the eight weeks prior to pre- or post titer were included. The median time to vaccination initiation was 13 months (range 6-66) post-CAR T. Pre and post-vaccination titers were available for 49 patients. Pre-vaccination seroprotection was high (> 85%) for tetanus and poliovirus. Among patients not seroprotected prior to vaccination, vaccine response rates were high for tetanus and polio (100%), moderate for diphtheria (75%) and haemophilus influenzae type b (62%), and lower for pertussis (48%), hepatitis A (43%), hepatitis B (44%), and pneumococcal disease (33%). CD19 CAR T recipients had higher pre-vaccination seroprotection rates than BCMA recipients, but vaccine responses did not differ significantly between groups. Pre-vaccination IgA levels were significantly associated with vaccine response, and absolute B-cell counts trended higher among responders (p = 0.054). Our findings highlight the importance of immune reconstitution in vaccine responses post-CAR T.
这项单中心回顾性研究分析了2018年至2024年间接受嵌合抗原受体(CAR)T细胞治疗后疫苗接种患者的疫苗反应。根据欧洲血液与骨髓移植协会(EBMT)/国际骨髓移植登记处(CIBMTR)的建议进行疫苗接种,并评估了对12种疫苗可预防感染的病原体特异性IgG反应。血清保护通过既定的临界值或滴度的显著倍数增加来定义。共有73例在滴度前或滴度后八周内未接受静脉注射免疫球蛋白的患者纳入研究。接种疫苗开始的中位时间为CAR T治疗后13个月(范围6 - 66个月)。49例患者有接种前和接种后的滴度数据。破伤风和脊髓灰质炎病毒的接种前血清保护率较高(> 85%)。在接种前未获得血清保护的患者中,破伤风和脊髓灰质炎的疫苗反应率较高(100%),白喉(75%)和b型流感嗜血杆菌(62%)的反应率中等,百日咳(48%)、甲型肝炎(43%)、乙型肝炎(44%)和肺炎球菌疾病(33%)的反应率较低。CD19 CAR T接受者的接种前血清保护率高于B细胞成熟抗原(BCMA)接受者,但两组之间的疫苗反应无显著差异。接种前IgA水平与疫苗反应显著相关,反应者的绝对B细胞计数有升高趋势(p = 0.054)。我们的研究结果强调了免疫重建在CAR T治疗后疫苗反应中的重要性。