Alqatta Wail
Ibn Sina Hospital, Sanaa, Yemen.
Int J Surg Case Rep. 2025 Aug;133:111643. doi: 10.1016/j.ijscr.2025.111643. Epub 2025 Jul 9.
Meckel's diverticulum (MD) is the most common congenital anomaly of the gastrointestinal tract, occurring in approximately 2 % of the population. While often asymptomatic, MD can occasionally lead to complications such as bleeding, inflammation, or small bowel obstruction (SBO). A rare cause of SBO involves a mesodiverticular band, an embryologic remnant capable of causing extrinsic compression or torsion. This condition remains under-recognized, especially in adolescents.
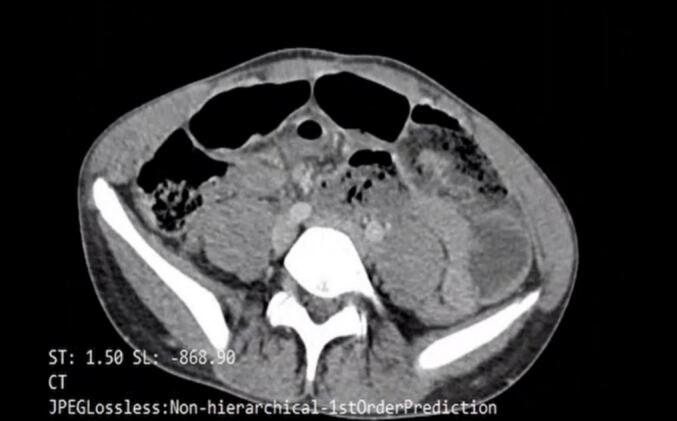
A 15-year-old male presented with acute abdominal pain, vomiting, and clinical signs of small bowel obstruction (SBO). Abdominal ultrasound and computed tomography (CT) revealed dilated small bowel loops with a distal transition point. CT imaging confirmed Meckel's diverticulitis in the right iliac fossa, associated with a mesodiverticular band, which was identified as the cause of the small bowel obstruction. Diagnostic laparoscopy confirmed the presence of a Meckel's diverticulitis with an associated mesodiverticular band causing torsion and obstruction. The band was divided with a harmonic scalpel, and the gangrenous diverticulum was resected laparoscopically using a linear endostapler. An appendectomy was also performed concurrently. The procedure was completed successfully without complications, and the patient was discharged in stable condition on postoperative day three.
Mesodiverticular bands are an uncommon but important etiology of small bowel obstruction in pediatric and adolescent patients. Their diagnosis is often delayed due to non-specific clinical and radiologic findings. Laparoscopy provides a dual benefit in such cases, allowing both definitive diagnosis and minimally invasive treatment with reduced morbidity.
This case underscores the need to consider Meckel's diverticulum and its associated bands in the differential diagnosis of SBO. Early laparoscopic intervention is both safe and effective, ensuring excellent outcomes.
梅克尔憩室(MD)是胃肠道最常见的先天性异常,发生率约为2%。MD通常无症状,但偶尔可导致出血、炎症或小肠梗阻(SBO)等并发症。SBO的一种罕见病因是中憩室带,这是一种胚胎残留结构,可导致外部压迫或扭转。这种情况仍未得到充分认识,尤其是在青少年中。
一名15岁男性因急性腹痛、呕吐及小肠梗阻(SBO)的临床体征就诊。腹部超声和计算机断层扫描(CT)显示小肠肠袢扩张,有一个远端移行点。CT成像证实右下腹有梅克尔憩室炎,伴有中憩室带,该中憩室带被确定为小肠梗阻的病因。诊断性腹腔镜检查证实存在梅克尔憩室炎,并伴有导致扭转和梗阻的中憩室带。用超声刀切断该带,并用线性切割吻合器腹腔镜切除坏疽性憩室。同时还进行了阑尾切除术。手术顺利完成,无并发症,患者术后第三天病情稳定出院。
中憩室带是小儿和青少年患者小肠梗阻的一种罕见但重要的病因。由于临床和影像学表现不具特异性,其诊断往往延迟。在这种情况下,腹腔镜检查有双重益处,既能明确诊断,又能进行微创治疗,降低发病率。
本病例强调在SBO的鉴别诊断中需考虑梅克尔憩室及其相关带。早期腹腔镜干预既安全又有效,可确保良好的治疗效果。