Thakir Tuba Mansoor, Wang Alice R, Decker-Farrell Amanda R, Ferrer Miriam, Guin Rohini N, Kleeman Sam, Levett Llewelyn, Zhao Xiang, Janowitz Tobias
Cold Spring Harbor Laboratory, Cold Spring Harbor, New York, USA.
Department of Pharmacological Sciences, Stony Brook University, Stony Brook, New York, USA.
J Clin Invest. 2025 Aug 1;135(15). doi: 10.1172/JCI191934.
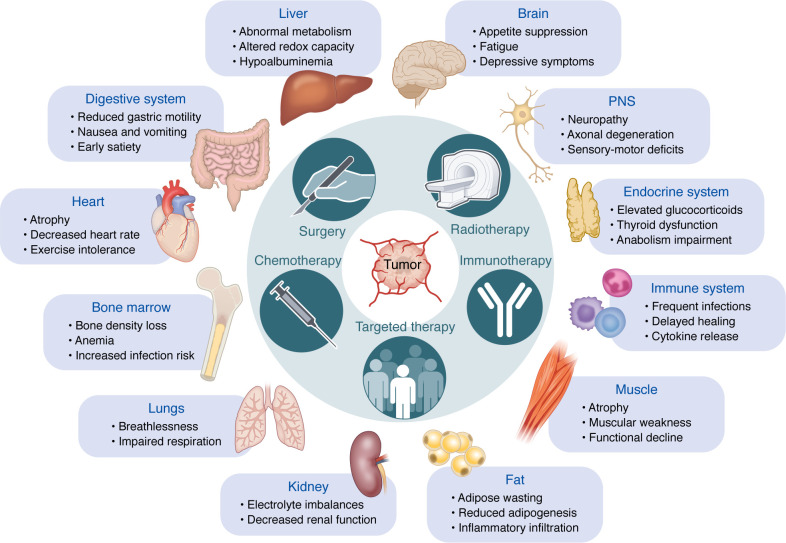
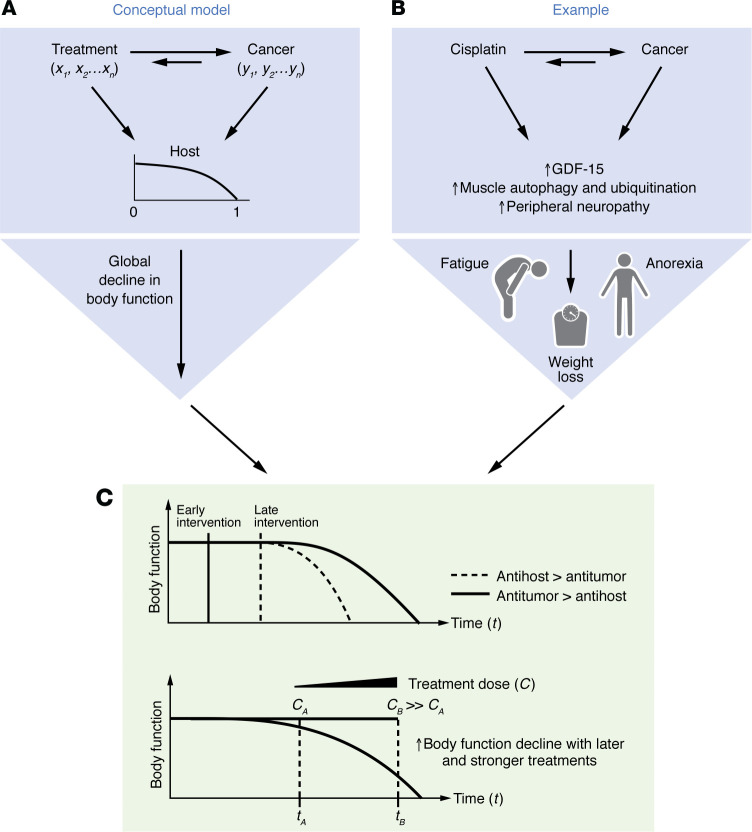
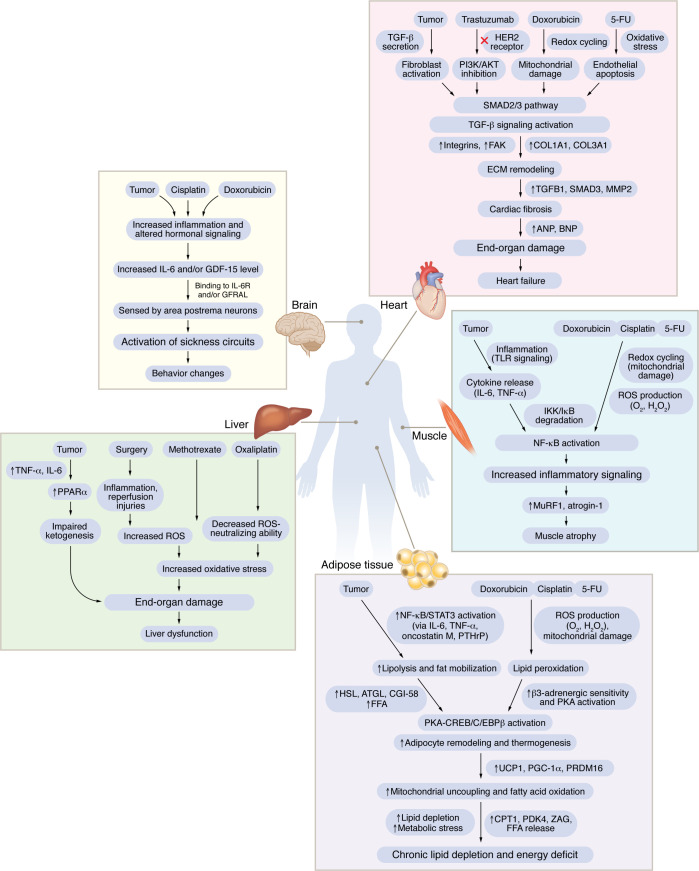
A central challenge in cancer therapy is the effective delivery of anticancer treatments while minimizing adverse effects on patient health. The potential dual impact of therapy is clearly illustrated in cancer-associated cachexia, a multifactorial syndrome characterized by involuntary weight loss, systemic inflammation, metabolic dysregulation, and behavioral alterations such as anorexia and apathy. While cachexia research often focuses on tumor-driven mechanisms, the literature indicates that cancer therapies themselves, particularly chemotherapies and targeted treatments, can initiate or exacerbate the biological pathways driving this syndrome. Here, we explore how therapeutic interventions intersect with the pathophysiology of cachexia, focusing on key organ systems including muscle, adipose tissue, liver, heart, and brain. We highlight examples such as therapy-induced upregulation of IL-6 and growth-differentiation factor 15, both contributing to reduced nutrient intake and a negative energy balance via brain-specific mechanisms. At the level of nutrient release and organ atrophy, chemotherapies also converge with cancer progression, for example, activating NF-κB in muscle and PKA/CREB signaling in adipose tissue. By examining how treatment timing and modality align with the natural trajectory of cancer cachexia, we underscore the importance of incorporating physiological endpoints alongside tumor-centric metrics in clinical trials. Such integrative approaches may better capture therapeutic efficacy while preserving patient well-being.
癌症治疗中的一个核心挑战是在将对患者健康的不良影响降至最低的同时,有效递送抗癌治疗。治疗的潜在双重影响在癌症相关性恶病质中得到了清晰体现,这是一种多因素综合征,其特征为非自愿体重减轻、全身炎症、代谢失调以及诸如厌食和冷漠等行为改变。虽然恶病质研究通常聚焦于肿瘤驱动的机制,但文献表明癌症治疗本身,尤其是化疗和靶向治疗,可启动或加剧驱动该综合征的生物学途径。在此,我们探讨治疗干预如何与恶病质的病理生理学相互作用,重点关注包括肌肉、脂肪组织、肝脏、心脏和大脑在内的关键器官系统。我们突出了一些例子,比如治疗诱导的白细胞介素-6和生长分化因子15上调,二者均通过脑特异性机制导致营养摄入减少和能量负平衡。在营养物质释放和器官萎缩层面,化疗也与癌症进展趋同,例如,激活肌肉中的核因子κB以及脂肪组织中的蛋白激酶A/环磷腺苷效应元件结合蛋白信号通路。通过研究治疗时机和方式如何与癌症恶病质的自然病程相匹配,我们强调在临床试验中将生理终点指标与以肿瘤为中心的指标相结合的重要性。这种综合方法可能在维护患者健康的同时,更好地评估治疗效果。