Guggilla Vijeeth, Pacheco Jennifer A, Carvalho Alexandre M, Whitmer Grant R, Pawlowski Anna E, Johnson Jodi L, Gao Catherine A, Achenbach Chad J, Walunas Theresa L
Institute for Artificial Intelligence in Medicine, Northwestern University Feinberg School of Medicine, Chicago, Illinois, United States of America.
Northwestern University Feinberg School of Medicine, Chicago, Illinois, United States of America.
PLoS One. 2025 Aug 8;20(8):e0330110. doi: 10.1371/journal.pone.0330110. eCollection 2025.
Adults with immunosuppression are more likely to develop severe COVID-19 than adults without immunosuppression. Less is known about differences in outcomes for adults with immunosuppression who are hospitalized with COVID-19.
A retrospective cohort study of adults hospitalized with COVID-19 at Northwestern Medicine hospitals between 03/01/2020 and 05/31/2022 was performed. Regression analyses were performed comparing in-hospital mortality, intensive care unit (ICU) admission, oxygenation requirements, and hospital/ICU length of stay among patients without immunosuppression (n = 9079) and patients with immunosuppression (n = 873).
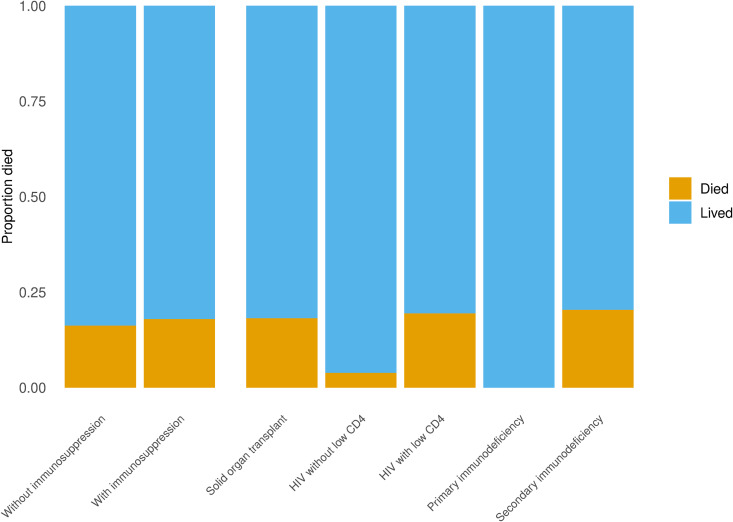
Patients with immunosuppression had significantly higher mortality than patients without immunosuppression (OR: 1.33, 95% CI: 1.11-1.60). This effect was even stronger when controlling for age at admission, diabetes, obesity, SARS-CoV-2 variant era, and COVID-19 medication use (adjusted OR: 1.78, 95% CI: 1.46-2.16). ICU admission (adjusted OR: 1.64, 95% CI: 1.41-1.90) and invasive ventilation (adjusted OR: 1.68, 95% CI: 1.36-2.06) were also significantly higher in patients with immunosuppression. Hospitalization length (median: 7 days) and ICU length of stay (median: 2.5 days) were longer in patients with immunosuppression compared to patients without immunosuppression (median: 5 days, adjusted p < 0.001; median: 2 days, adjusted p = 0.04). Subgroup analyses showed that patients with solid organ transplant, HIV with low CD4 cell count, and secondary immunodeficiency had significantly higher adjusted mortality and ICU admission compared to patients without immunosuppression. Patients with solid organ transplant also had significantly higher invasive ventilation and ICU length of stay.
Patients with immunosuppression had worse outcomes than patients without immunosuppression. Subgroup analyses showed that patients with solid organ transplant had the worst outcomes overall. Patients with HIV had similar outcomes as patients without immunosuppression unless CD4 cell count was low.
免疫功能低下的成年人比免疫功能正常的成年人更易发展为重症 COVID-19。对于因 COVID-19 住院的免疫功能低下成年人的预后差异,人们了解较少。
对 2020 年 3 月 1 日至 2022 年 5 月 31 日期间在西北大学医学院各医院因 COVID-19 住院的成年人进行了一项回顾性队列研究。进行回归分析,比较免疫功能正常患者(n = 9079)和免疫功能低下患者(n = 873)的院内死亡率、重症监护病房(ICU)入住率、氧疗需求以及住院/ICU 住院时长。
免疫功能低下患者的死亡率显著高于免疫功能正常患者(比值比:1.33,95% 置信区间:1.11 - 1.60)。在控制入院年龄、糖尿病、肥胖、SARS-CoV-2 变异株流行时期以及 COVID-19 用药情况后,这种效应更强(校正比值比:1.78,95% 置信区间:1.46 - 2.16)。免疫功能低下患者的 ICU 入住率(校正比值比:1.64,95% 置信区间:1.41 - 1.90)和有创通气率(校正比值比:1.68,95% 置信区间:1.36 - 2.06)也显著更高。与免疫功能正常患者相比,免疫功能低下患者的住院时长(中位数:7 天)和 ICU 住院时长(中位数:2.5 天)更长(免疫功能正常患者中位数:5 天,校正 p < 0.001;中位数:2 天,校正 p = 0.04)。亚组分析显示,与免疫功能正常患者相比,实体器官移植患者、CD4 细胞计数低的 HIV 患者以及继发性免疫缺陷患者的校正死亡率和 ICU 入住率显著更高。实体器官移植患者的有创通气率和 ICU 住院时长也显著更高。
免疫功能低下患者的预后比免疫功能正常患者更差。亚组分析显示,实体器官移植患者的总体预后最差。HIV 患者的预后与免疫功能正常患者相似,除非 CD4 细胞计数低。