Wu Xianfeng, Lin Wenjun, Zhao Jinyuan, Tian Na, Xu Qingdong, Wen Yueqiang, Zhan Xiaojiang, Peng Fenfen, Wang Xiaoyang, Su Ning, Feng Xiaoran, Wang Niansong, Wu Juan
Department of Nephrology, Shanghai Jiao Tong University Affiliated Sixth People's Hospital, No.600, Yi Shan Road, Shanghai, 200233, China.
Department of Nephrology, Shanghai Eighth People's Hospital, Shanghai, 200235, China.
Sci Rep. 2025 Aug 12;15(1):29473. doi: 10.1038/s41598-025-15473-z.
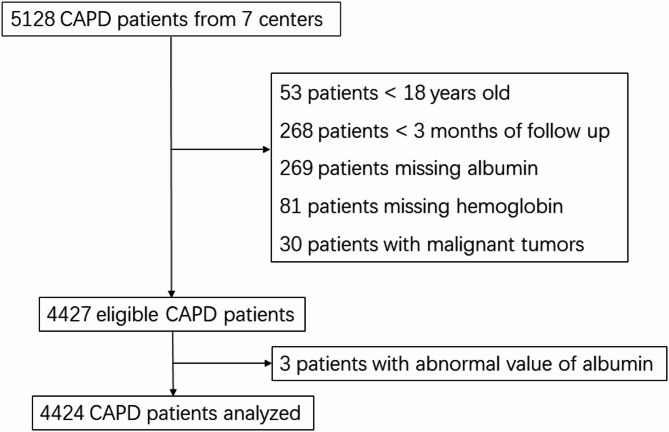
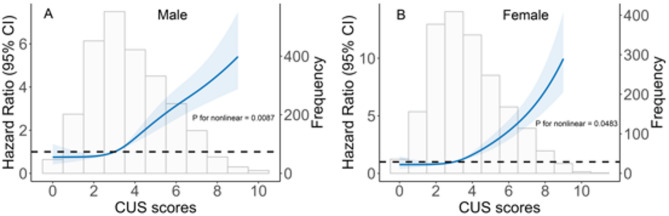
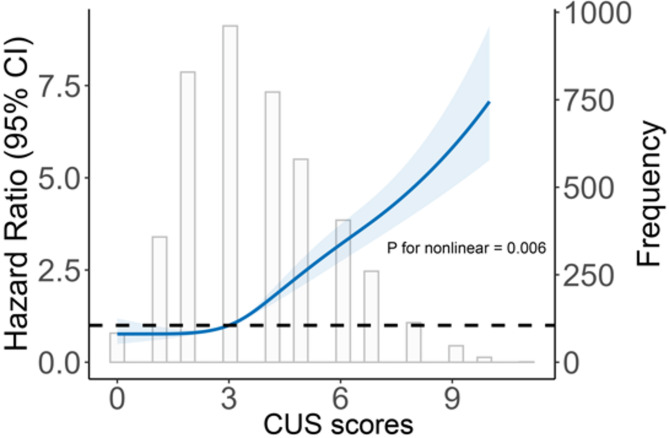
No study has comprehensively investigated the association between comorbidities, uremic-specific complications (collectively defined as clinical uremic syndrome [CUS]), and mortality in peritoneal dialysis (PD) patients. We conducted a retrospective cohort study including 4,424 incident PD patients from seven centers in China. Comorbidities and complications were each assigned one point: cardiovascular disease, peripheral vascular disease, cerebrovascular disease, diabetes mellitus, hypertension, hyperlipidemia, malnutrition, and anemia. Patients aged 50 years or older received additional points. The total score (CUS score) was calculated to evaluate its association with mortality in PD patients. Over 18,898.4 person-years of follow-up, 1,208 patients (27.3%) died. The median CUS score was 3 (interquartile range [IQR] 2-5; range, 1-11). A nonlinear association between CUS scores and all-cause mortality was observed (nonlinear, p = 0.006). A pre-1point increase in the CUS score was associated with a 1.35-fold increase in the risk of all-cause mortality (95% confidence interval [CI], 1.31-1.39). Compared with patients with CUS scores ≤ 3, those with scores > 3 had a 2.81-fold higher risk of mortality (95% CI, 2.47-3.21). Higher CUS scores were significantly associated with increased all-cause mortality risk in PD patients, particularly those with scores > 3.
尚无研究全面调查过合并症、尿毒症特异性并发症(统称为临床尿毒症综合征[CUS])与腹膜透析(PD)患者死亡率之间的关联。我们进行了一项回顾性队列研究,纳入了来自中国七个中心的4424例新发PD患者。合并症和并发症各计1分:心血管疾病、外周血管疾病、脑血管疾病、糖尿病、高血压、高脂血症、营养不良和贫血。年龄在50岁及以上的患者额外计分。计算总分(CUS评分)以评估其与PD患者死亡率的关联。在超过18898.4人年的随访期内,1208例患者(27.3%)死亡。CUS评分的中位数为3(四分位间距[IQR]2 - 5;范围,1 - 11)。观察到CUS评分与全因死亡率之间存在非线性关联(非线性,p = 0.006)。CUS评分每增加1分,全因死亡风险增加1.35倍(95%置信区间[CI],1.31 - 1.39)。与CUS评分≤3的患者相比,评分>3的患者死亡风险高2.81倍(95%CI,2.47 - 3.21)。较高的CUS评分与PD患者全因死亡风险增加显著相关,尤其是评分>3的患者。