Dung Tran Thi Ngoc, Vinh Chau, Anh Pham Hong, Linh Vo Kim Phuong, Tuyen Ha Thanh, Tam Pham Thanh, Lan Nguyen Phu Huong, Phu Truong Thien, Tuyet Nguyen Su Minh, Nhung Pham Hong, Trang Van Dinh, Van Nguyen Thi, Nguyen Quynh, Thanh Nguyen Thi, Kesteman Thomas, van Doorn H Rogier, Thwaites Guy, Duy Pham Thanh
Molecular Epidemiology Group, Oxford University Clinical Research Unit, Ho Chi Minh City, Vietnam.
Hospital for Tropical Diseases, Ho Chi Minh City, Vietnam.
Ann Clin Microbiol Antimicrob. 2025 Aug 31;24(1):50. doi: 10.1186/s12941-025-00818-3.
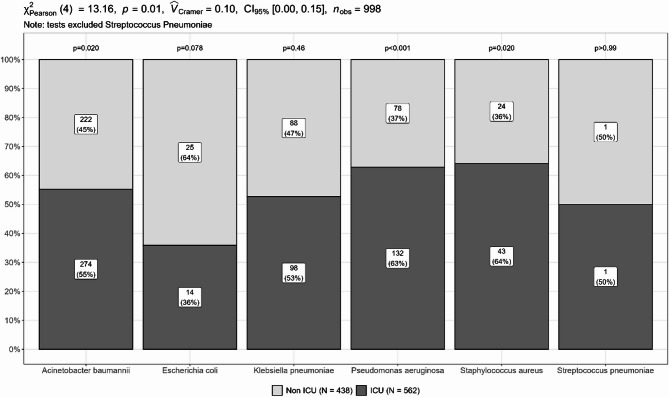
Lower respiratory tract infection (LRTI) remains the leading infectious cause of morbidity and mortality globally. Key bacterial pathogens include Acinetobacter baumannii, Pseudomonas aeruginosa, Klebsiella pneumoniae, Escherichia coli, Staphylococcus aureus and Streptococcus pneumoniae. This study examined the prevalence and antimicrobial resistance patterns of major bacterial pathogens from community- and hospital-acquired LRTIs across six major hospitals in Vietnam.
Between January 2022 and May 2023, 1000 bacterial isolates were collected through an isolate-based surveillance. Species identification and antimicrobial susceptibility testing were performed by VITEK-2/Phoenix M50, with MICs determined by E-test or broth microdilution. Multiplex PCRs were used to detect common AMR genes.
A. baumannii (49.6%), P. aeruginosa (21%), K. pneumoniae (18.6%) were predominant, followed by S. aureus (6.7%), E. coli (3.9%) and S. pneumoniae (0.2%). Most isolates (94.4%) were identified from hospital-acquired cases. High prevalence of MDR and carbapenem resistance were identified in A. baumannii (96% and 95%), P. aeruginosa (56.7% and 57.1%), and K. pneumoniae (78% and 69.2%), respectively. Notably, resistance to ceftazidime-avibactam was detected in K. pneumoniae (34.3%), P. aeruginosa (29%), and E. coli (7.7%), while colistin resistance was found in K. pneumoniae (18.2%) and A. baumannii (2.8%). MRSA prevalence was 79.1%, though S. aureus remained susceptible to vancomycin, linezolid and ceftaroline. Most bla-positive K. pneumoniae (62/71, 87.3%), E. coli (2/2, 100%), and P. aeruginosa (23/25, 85.2%) showed resistance to ceftazidime-avibactam. Whole genome sequencing revealed that the bla-positive but ceftazidime-avibactam susceptible isolates (9 K. pneumoniae and 2 P. aeruginosa) carried truncated bla. Overall, ceftazidime-avibactam was effective against K. pneumoniae, E. coli, and P. aeruginosa isolates carrying ESBL, ESBL and bla, or ESBL and bla. Alternatively, no detectable AMR genes were found in 35 ceftazidime-avibactam resistant P. aeruginosa isolates.
Carbapenem-resistant Gram-negative pathogens were predominant among hospital-acquired LRTIs in Vietnam, with notable resistance to ceftazidime-avibactam and colistin. The lack of effective treatment for A. baumannii remains a major concern. We found a strong correlation between AMR phenotype and genotype among K. pneumoniae and E. coli, supporting gene-based therapy to guide ceftazidime-avibactam use. However, the presence of disrupted bla underscores the need to re-evaluate commercial PCR assays for carbapenemase detection.
下呼吸道感染(LRTI)仍是全球发病和死亡的主要感染原因。主要细菌病原体包括鲍曼不动杆菌、铜绿假单胞菌、肺炎克雷伯菌、大肠埃希菌、金黄色葡萄球菌和肺炎链球菌。本研究调查了越南六家主要医院社区获得性和医院获得性LRTIs中主要细菌病原体的流行情况和抗菌药物耐药模式。
2022年1月至2023年5月期间,通过基于分离株的监测收集了1000株细菌分离株。采用VITEK-2/Phoenix M50进行菌种鉴定和抗菌药物敏感性试验,通过E-test或肉汤微量稀释法测定最低抑菌浓度(MIC)。采用多重聚合酶链反应(PCR)检测常见的耐药基因。
鲍曼不动杆菌(49.6%)、铜绿假单胞菌(21%)、肺炎克雷伯菌(18.6%)占主导地位,其次是金黄色葡萄球菌(6.7%)、大肠埃希菌(3.9%)和肺炎链球菌(0.2%)。大多数分离株(94.4%)来自医院获得性病例。鲍曼不动杆菌(96%和95%)、铜绿假单胞菌(56.7%和57.1%)和肺炎克雷伯菌(78%和69.2%)中多重耐药和碳青霉烯耐药的发生率较高。值得注意的是,肺炎克雷伯菌(34.3%)、铜绿假单胞菌(29%)和大肠埃希菌(7.7%)中检测到对头孢他啶-阿维巴坦的耐药性,而肺炎克雷伯菌(18.2%)和鲍曼不动杆菌(2.8%)中发现对黏菌素的耐药性。耐甲氧西林金黄色葡萄球菌(MRSA)的患病率为79.1%,尽管金黄色葡萄球菌对万古霉素、利奈唑胺和头孢洛林仍敏感。大多数产bla的肺炎克雷伯菌(62/71,87.3%)、大肠埃希菌(2/2,100%)和铜绿假单胞菌(23/25,85.2%)对头孢他啶-阿维巴坦耐药。全基因组测序显示,产bla但对头孢他啶-阿维巴坦敏感的分离株(9株肺炎克雷伯菌和2株铜绿假单胞菌)携带截短的bla。总体而言,头孢他啶-阿维巴坦对携带超广谱β-内酰胺酶(ESBL)、ESBL和bla或ESBL和bla的肺炎克雷伯菌、大肠埃希菌和铜绿假单胞菌分离株有效。另外,在35株对头孢他啶-阿维巴坦耐药的铜绿假单胞菌分离株中未检测到可检测的耐药基因。
耐碳青霉烯革兰阴性病原体在越南医院获得性LRTIs中占主导地位,对头孢他啶-阿维巴坦和黏菌素具有显著耐药性。鲍曼不动杆菌缺乏有效治疗仍然是一个主要问题。我们发现肺炎克雷伯菌和大肠埃希菌的耐药表型与基因型之间存在很强的相关性,支持基于基因的疗法来指导头孢他啶-阿维巴坦的使用。然而,截短的bla的存在强调了重新评估用于碳青霉烯酶检测的商业PCR检测方法的必要性。