McKillop J H
West J Med. 1980 Jul;133(1):26-43.
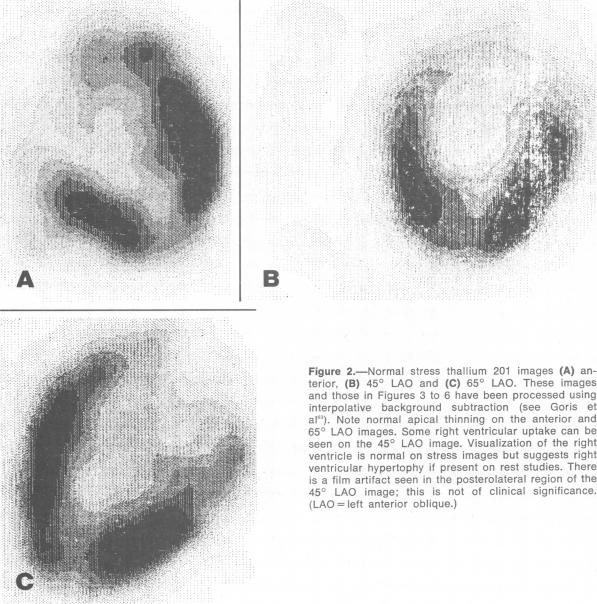
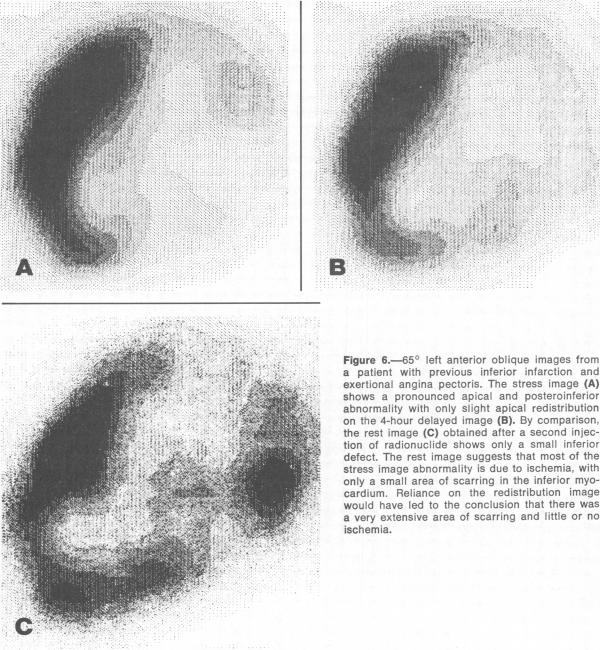
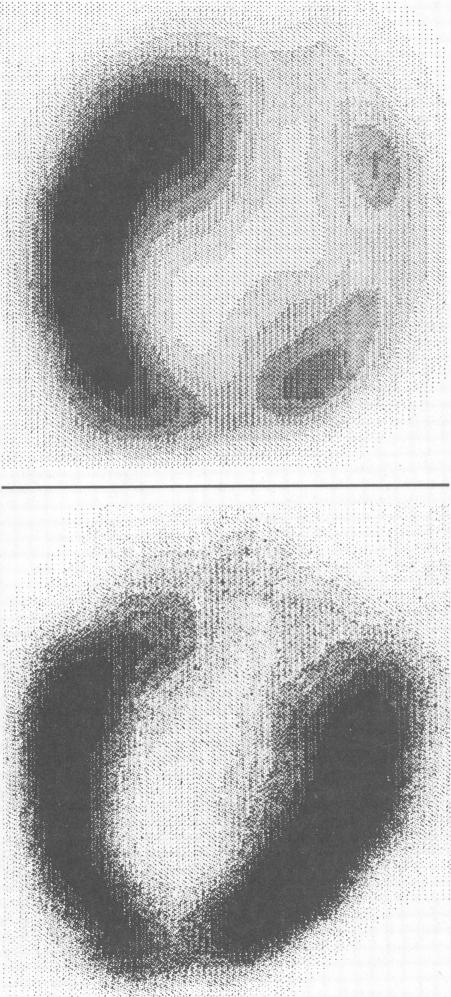
The radioactive isotope thallium 201 behaves physiologically as a potassium analog, and when injected intravenously accumulates rapidly within the cells of many organs. Uptake of the isotope reflects both regional perfusion and sodium-potassium pump activity. The radionuclide emits 80 keV x-rays which are suitable for scintillation camera imaging. The main clinical application of (201)TI scintigraphy has been in myocardial imaging. Abnormal uptake of the isotope results in a cold spot on the myocardial image. In patients with coronary artery disease, the differentiation of ischemic and infarcted myocardium is made by comparing images obtained after injecting the radionuclide at the peak of a maximal exercise test with those obtained after injection at rest. Abnormalities due to ischemia usually are seen only on the stress image whereas fixed defects in both rest and stress studies usually indicate areas of infarction or scarring. Some investigators believe that redistribution images obtained four to six hours after stress injection (without administering further (201)TI) give the same information as a separate rest study. The sensitivity of stress imaging for detecting significant coronary disease is of the order of 80 percent to 95 percent, though computer processing of the images may be necessary to achieve the higher figure. The prediction of the extent of coronary disease from (201)TI images is less reliable. An abnormal (201)TI image is not entirely specific for coronary artery disease and the likelihood of an abnormal image being due to this diagnosis varies according to the clinical circumstances. The main clinical value of (201)TI myocardial imaging is likely to be in the noninvasive screening of patients with atypical chest pain or with ambiguous findings on stress electrocardiographic tests. It has also proved useful in studying patients with variant angina or following a coronary bypass operation. It is doubtful whether the technique is clinically helpful in most patients with suspected or established acute myocardial infarction. Imaging of organs other than the heart with (201)TI has received much less attention but has been reported in patients with peripheral vascular disease and various primary and secondary neoplasms.
放射性同位素铊201在生理上表现为钾的类似物,静脉注射后能迅速在许多器官的细胞内蓄积。该同位素的摄取反映了局部灌注和钠钾泵活性。这种放射性核素发射适合闪烁相机成像的80keV X射线。铊201心肌闪烁显像的主要临床应用是心肌成像。该同位素的异常摄取会在心肌图像上形成冷区。在冠心病患者中,通过比较在最大运动试验峰值时注射放射性核素后获得的图像与静息时注射后获得的图像,来区分缺血心肌和梗死心肌。缺血导致的异常通常仅在负荷图像上可见,而静息和负荷研究中的固定缺损通常提示梗死或瘢痕区域。一些研究者认为,负荷注射后4至6小时获得的再分布图像(不再给予铊201)与单独的静息研究提供相同的信息。负荷成像检测显著冠状动脉疾病的敏感性约为80%至95%,不过可能需要对图像进行计算机处理才能达到较高的数值。根据铊201图像预测冠状动脉疾病的程度不太可靠。异常的铊201图像并非完全特异性地提示冠状动脉疾病,且该诊断导致图像异常的可能性因临床情况而异。铊201心肌成像的主要临床价值可能在于对非典型胸痛或负荷心电图检查结果不明确的患者进行无创筛查。它在研究变异型心绞痛患者或冠状动脉搭桥手术后的患者方面也已证明是有用的。对于大多数疑似或确诊为急性心肌梗死的患者,该技术在临床上是否有帮助尚不确定。用铊201对心脏以外的器官进行成像受到的关注要少得多,但已在周围血管疾病以及各种原发性和继发性肿瘤患者中有所报道。