Gayowski T J, Marino I R, Doyle H R, Echeverri L, Mieles L, Todo S, Wagener M, Singh N, Yu V L, Fung J J, Starzl T E
Veterans Administration Medical Center, Pittsburgh, Pennsylvania 15213, USA.
J Surg Res. 1996 Feb 1;60(2):333-8. doi: 10.1006/jsre.1996.0053.
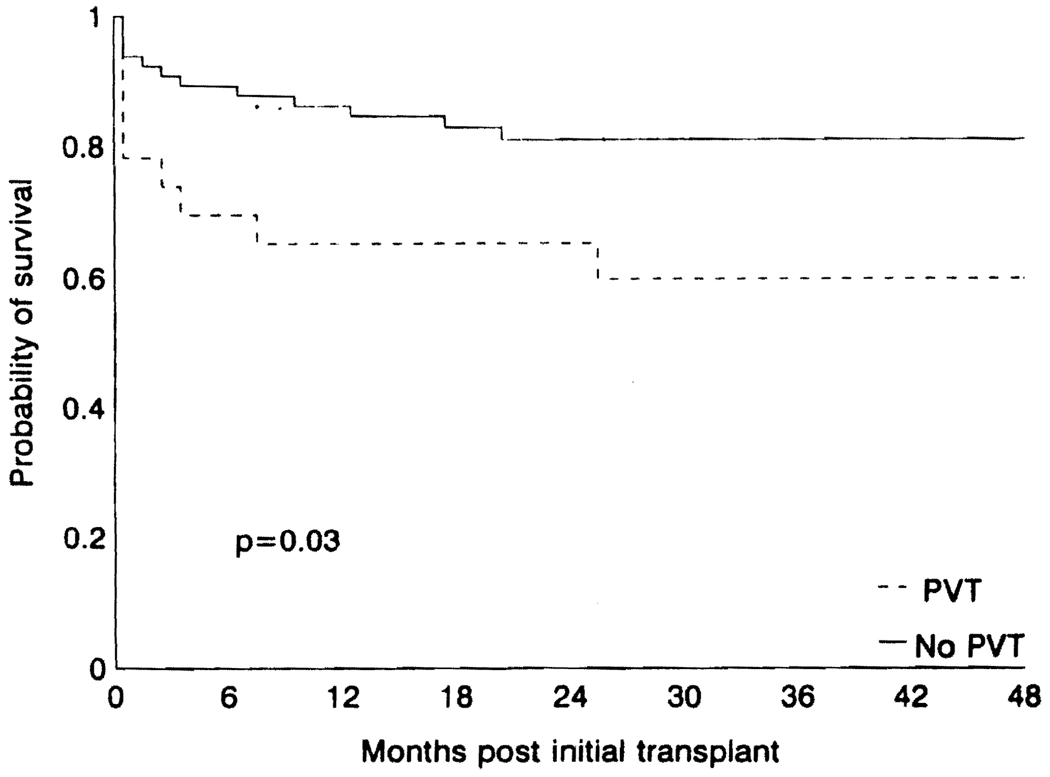
The incidence of native portal vein thrombosis (PVT) in liver transplant recipients has been reported to range from 2.1 to 13.8%. We have identified an inordinately high incidence of PVT in a consecutive series of U.S. veterans receiving liver transplants. Between October 1989 and February 1994, 88 consecutive U.S. veterans received 99 orthotopic liver transplants under primary Tacrolimus (Prograf, formerly FK506) based immunosuppression. A number of clinical features were examined in an effort to identify risk factors for PVT and outcome was compared to patients without PVT. Native PVT was present in 23/88 (26%) patients. All of these patients were male U.S. veterans with a mean age of 47 years. When compared to the 65 patients without PVT, we found no significant difference with respect to underlying liver disease, age, Childs-Pugh score (mean = 12), UNOS status as defined prior to April 1995 (95% UNOS 3 or 4), previous abdominal surgery, or liver volume. Median blood loss for patients with PVT (21 units of packed red blood cells) was greater than for those without PVT (14 units, P = 0.04). Portal thrombectomy was performed in 11 patients, 11 patients required mesoportal jump grafts, and 1 patient had an interposition graft. Standard veno-venous bypass was used in 10 patients with single bypass utilized for the remainder. Actuarial patient survival for all patients at 1, 2, and 4 years was 88, 85, and 79%, respectively. There was no significant difference in patients with or without PVT. Patients with PVT had poorer graft survival than patients without PVT (86% vs 65%, 1 year; 81% vs 65%, 2 years; 81% vs 61%, 4 years; P = 0.03); however, this was not related to technical problems with the portal venous inflow. PVT occurred in 26% of U.S. veterans undergoing liver transplantation. These patients had significantly higher operative blood loss and poorer graft survival. The high incidence of postnecrotic cirrhosis in a predominantly male group of patients with advanced disease, as is evident by the high mean Childs-Pugh score and UNOS status, perhaps accounts for our observations.
据报道,肝移植受者中天然门静脉血栓形成(PVT)的发生率在2.1%至13.8%之间。我们发现,在美国连续接受肝移植的退伍军人中,PVT的发生率异常高。1989年10月至1994年2月期间,88名连续的美国退伍军人在以他克莫司(普乐可复,原FK506)为主的免疫抑制下接受了99例原位肝移植。我们检查了一些临床特征,以确定PVT的危险因素,并将结果与无PVT的患者进行比较。88例患者中有23例(26%)存在天然PVT。所有这些患者均为美国男性退伍军人,平均年龄47岁。与65例无PVT的患者相比,我们发现他们在潜在肝病、年龄、Childs-Pugh评分(平均=12)、1995年4月之前定义的UNOS状态(95%为UNOS 3或4)、既往腹部手术或肝脏体积方面没有显著差异。PVT患者的中位失血量(21单位浓缩红细胞)高于无PVT的患者(14单位,P=0.04)。11例患者进行了门静脉血栓切除术,11例患者需要进行肠系膜门静脉搭桥术,1例患者进行了间置移植。10例患者使用了标准的静脉-静脉旁路,其余患者使用了单旁路。所有患者1年、2年和4年的精算生存率分别为88%、85%和79%。有PVT和无PVT的患者之间没有显著差异。有PVT的患者的移植物生存率低于无PVT的患者(1年时为86%对65%;2年时为81%对65%;4年时为81%对61%;P=0.03);然而,这与门静脉流入的技术问题无关。接受肝移植的美国退伍军人中有26%发生了PVT。这些患者的手术失血量明显更高,移植物生存率更低。正如高平均Childs-Pugh评分和UNOS状态所显示的那样,在一组以男性为主的晚期疾病患者中,坏死性肝硬化的发生率很高,这可能解释了我们的观察结果。