Harris G J, Garcia G H, Logani S C, Murphy M L, Sheth B P, Seth A K
Department of Ophthalmology, Medical College of Wisconsin, Milwaukee, USA.
Trans Am Ophthalmol Soc. 1998;96:329-47; discussion 347-53.
BACKGROUND/PURPOSE: Although the management of orbital blow-out fractures was controversial for many years, refined imaging with computed tomography (CT) helped to narrow the poles of the debate. Many orbital surgeons currently recommend repair if fracture size portends late enophthalmos, or if diplopia has not substantially resolved within 2 weeks of the injury. While volumetric considerations have been generally well-served by this approach, ocular motility outcomes have been less than ideal. In one series, almost 50% of patients had residual diplopia 6 months after surgery. A fine network of fibrous septa that functionally unites the periosteum of the orbital floor, the inferior fibrofatty tissues, and the sheaths of the inferior rectus and oblique muscles was demonstrated by Koornneef. Entrapment between bone fragments of any of the components of this anatomic unit can limit ocular motility. Based on the pathogenesis of blow-out fractures, in which the fibrofatty-muscular complex is driven to varying degrees between bone fragments, some measure of soft tissue damage might be anticipated. Subsequent intrinsic fibrosis and contraction can tether globe movement, despite complete reduction of herniated orbital tissue from the fracture site. We postulated that the extent of this soft tissue damage might be estimated from preoperative imaging studies.
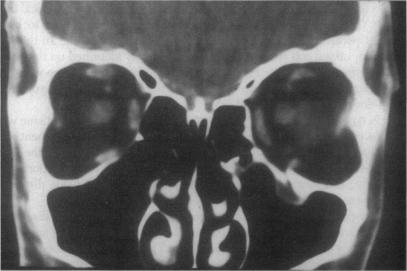
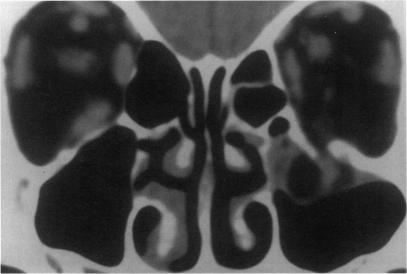
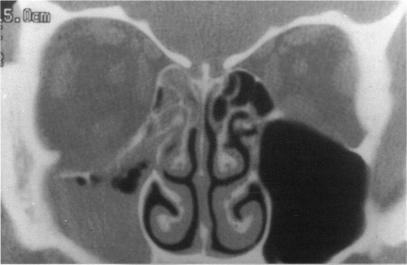
Study criteria included: retrievable coronal CT scans; fractures of the orbital floor without rim involvement, with or without extension into the medial wall; preoperative diplopia; surgical repair by a single surgeon; complete release of entrapped tissues; and postoperative ocular motility outcomes documented with binocular visual fields (BVFs). Thirty patients met all criteria. The CT scans and BVFs were assessed by different examiners among the authors. Fractures were classified into 3 general categories and 2 subtypes to reflect the severity of soft tissue damage within each category. "Trap-door" injuries, in which bone fragments appeared to have almost perfectly realigned, were classified as type I fractures. In the I-A subtype, no orbital tissue was visible on the sinus side of the fracture line. In the I-B subtype, soft tissue with the radiodensity of orbital fat was visible within the maxillary sinus. In type II fractures, bone fragments were distracted and soft tissue was displaced between them. In the II-A subtype, soft tissue displacement was less than, or proportional to, bone fragment distraction. In the II-B subtype, soft tissue displacement was greater than bone fragment distraction. In type III fractures, displaced bone fragments surrounded displaced soft tissue in all areas. In the III-A subtype, soft tissue and bone were moderately displaced. In the III-B subtype, both were markedly displaced. Motility outcomes were quantified by measuring the vertical excursion in BVFs. The interval between trauma and surgical repair was also determined.
Among the 15 patients with a motility outcome in BVFs which was poorer than the median (86 degrees or less of single binocular vertical excursion), 4 patients (27%) had type A fractures; 11 patients (73%) had type B fractures. Among the 15 patients with a better outcome than the median (88 degrees or more), 10 patients (67%) had type A fractures; 5 patients (33%) had type B fractures. These differences became more defined as analysis moved away from the median. Among 5 patients with type B fractures and better than the median result in BVFs, 3 patients (60%) had surgical repair during the first week after injury. Among the 11 patients with type B fractures and less than the median result, 1 patient (9%) had repair during the first week.
When the CT-depicted relationship between bone fragments and soft tissues is considered, a wide spectrum of injuries is subsumed under the rubric of blow-out fractures. In general, greater degrees of soft tissue incarceration or displacement, with presumably greater intrinsic damage and subsequent fibrosis, appear to result in poorer motility outcomes. Although this retrospective study does not conclusively prove its benefit, an urgent surgical approach to selected injuries should be considered.

背景/目的:尽管眼眶爆裂性骨折的治疗多年来一直存在争议,但计算机断层扫描(CT)的精细成像有助于缩小争论的范围。目前,许多眼眶外科医生建议,如果骨折大小预示会出现晚期眼球内陷,或者如果复视在受伤后2周内没有明显缓解,就进行修复。虽然这种方法在容积方面的考虑总体上效果良好,但眼球运动结果并不理想。在一个系列研究中,近50%的患者术后6个月仍有残余复视。Koornneef证实存在一个精细的纤维间隔网络,它在功能上连接眶底骨膜、眶下纤维脂肪组织以及下直肌和下斜肌鞘。该解剖单元任何组成部分被骨碎片卡压都可能限制眼球运动。基于爆裂性骨折的发病机制,即纤维脂肪 - 肌肉复合体在不同程度上被挤入骨碎片之间,可以预期会有一定程度的软组织损伤。尽管从骨折部位完全还纳了突出的眼眶组织,但随后的内在纤维化和收缩仍可能束缚眼球运动。我们推测这种软组织损伤的程度可以通过术前影像学研究来估计。
研究标准包括:可获取的冠状位CT扫描;眶底骨折不累及眶缘,可伴有或不伴有向内侧壁延伸;术前有复视;由单一外科医生进行手术修复;完全松解卡压的组织;以及通过双眼视野(BVF)记录术后眼球运动结果。30例患者符合所有标准。作者中的不同检查者对CT扫描和BVF进行评估。骨折分为3个一般类别和2个亚型,以反映每个类别中软组织损伤的严重程度。“活板门”损伤,即骨碎片似乎几乎完全重新对齐,被归类为I型骨折。在I - A亚型中,骨折线鼻窦侧看不到眶组织。在I - B亚型中,上颌窦内可见密度与眶脂肪相同的软组织。在II型骨折中,骨碎片分离,软组织在其间移位。在II - A亚型中,软组织移位小于或与骨碎片分离程度成比例。在II - B亚型中,软组织移位大于骨碎片分离程度。在III型骨折中,移位的骨碎片在所有区域围绕移位的软组织。在III - A亚型中,软组织和骨中等程度移位。在III - B亚型中,两者均明显移位。通过测量BVF中的垂直偏移来量化运动结果。还确定了受伤与手术修复之间的间隔时间。
在15例BVF运动结果比中位数差(单眼双眼垂直偏移86度或更小)的患者中,4例(27%)为A型骨折;11例(73%)为B型骨折。在15例结果比中位数好(88度或更大)的患者中,10例(67%)为A型骨折;5例(33%)为B型骨折。随着分析偏离中位数,这些差异变得更加明显。在5例BVF结果比中位数好的B型骨折患者中,3例(60%)在受伤后第一周内进行了手术修复。在11例结果低于中位数的B型骨折患者中,1例(9%)在第一周内进行了修复。
当考虑CT显示的骨碎片与软组织之间的关系时,爆裂性骨折这一类别涵盖了广泛的损伤情况。一般来说,软组织嵌顿或移位程度越大,可能内在损伤和随后的纤维化就越严重,似乎会导致更差的运动结果。尽管这项回顾性研究没有确凿证明其益处,但对于某些选定的损伤,应考虑采取紧急手术方法。