Knox D L, Kerrison J B, Green W R
W. Richard Green Eye Pathology Laboratory, Wilmer Institute, and Department of Pathology, Johns Hopkins Medical Institution, Baltimore, USA.
Trans Am Ophthalmol Soc. 2000;98:203-20; discussion 221-2.
To define the histopathologic features of eyes in which a pathologic diagnosis of ischemic optic neuropathy had been made in the years 1951 through 1998.
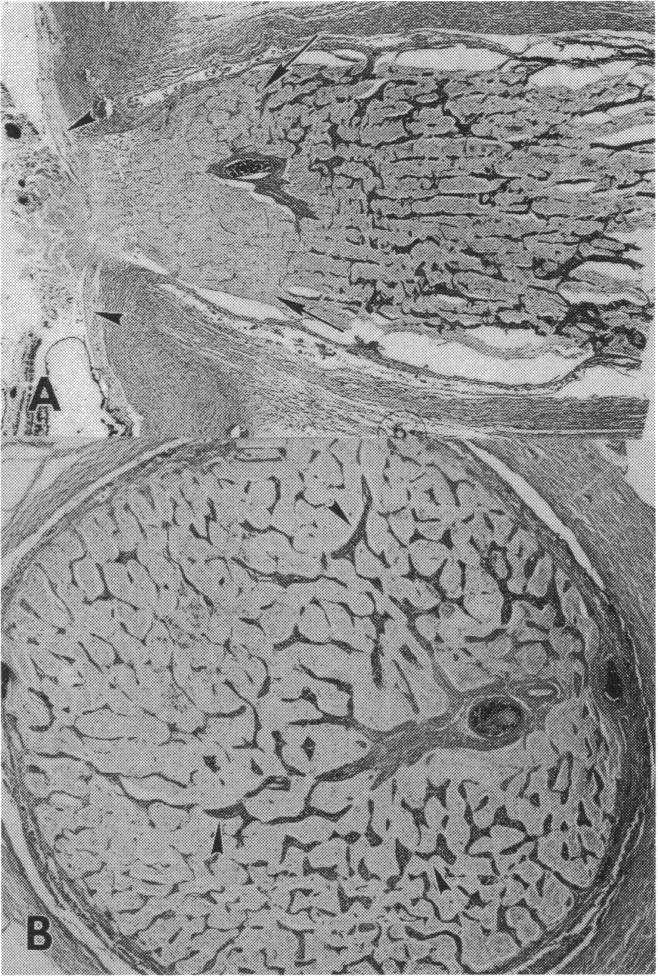
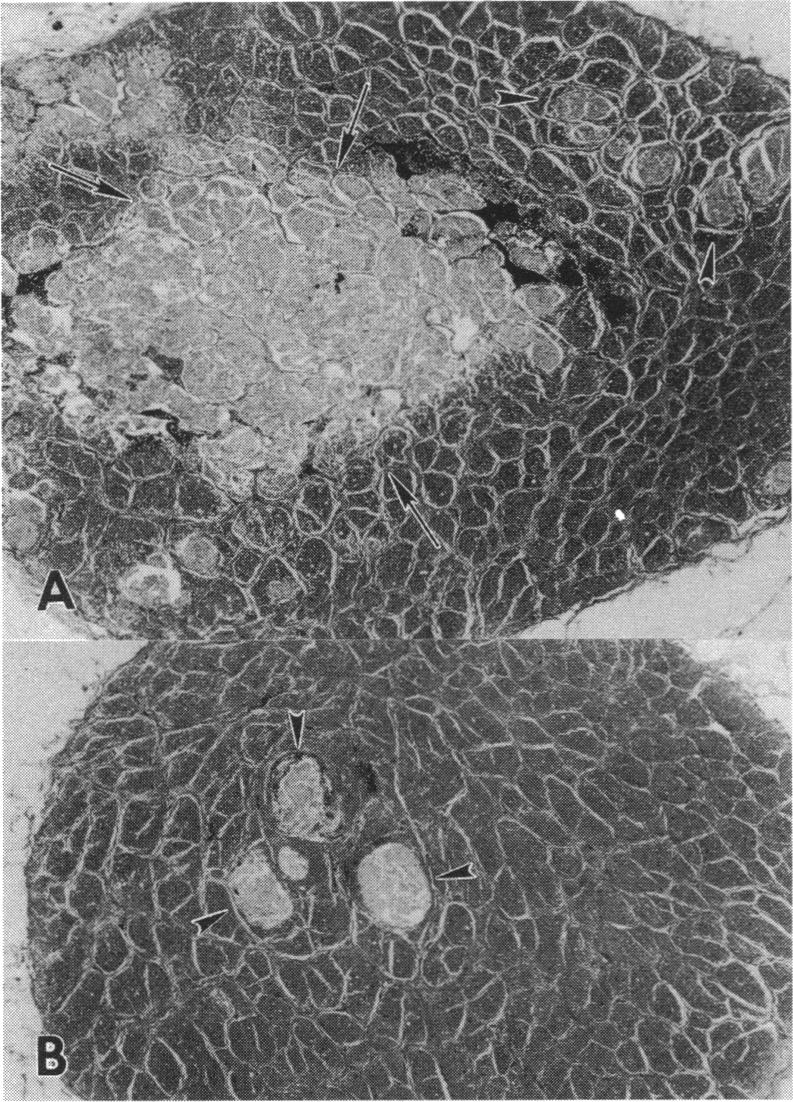
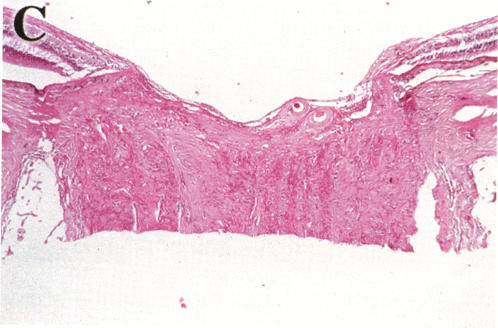
The following data were documented: age of patient, race, sex, source of tissue, cause of death, clinical history, interval from loss of vision to death, enucleation, exenteration, and biopsy. The histopathologic criteria for diagnosis of ischemic optic neuropathy were the presence of localized ischemic edema, cavernous degeneration, or an area of atrophy located superior or inferior in the optic nerve. Cases with history of abrupt loss of vision were combined with reports from the literature to construct a time table of histopathologic features and associated conditions.
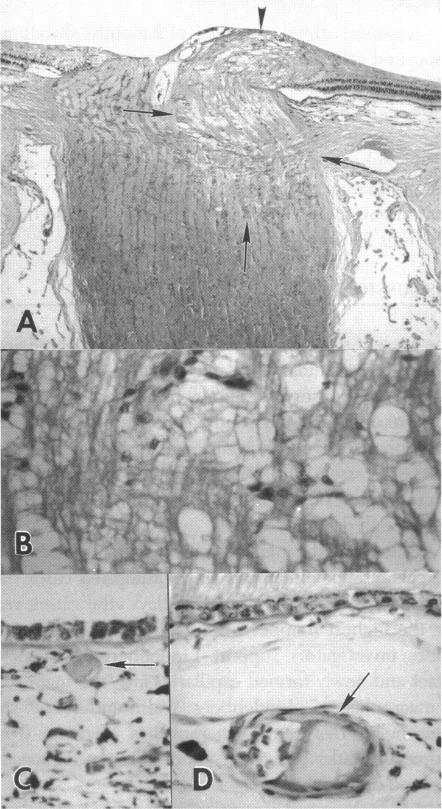
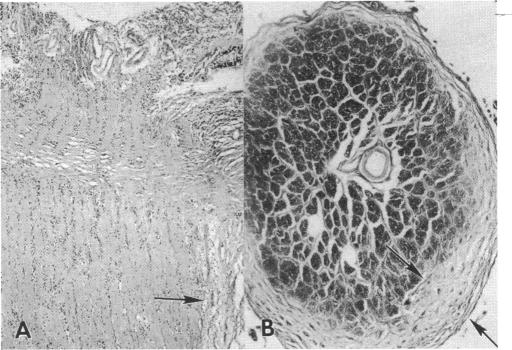
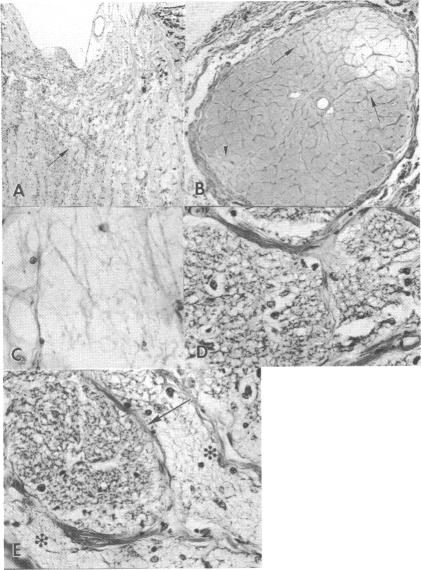
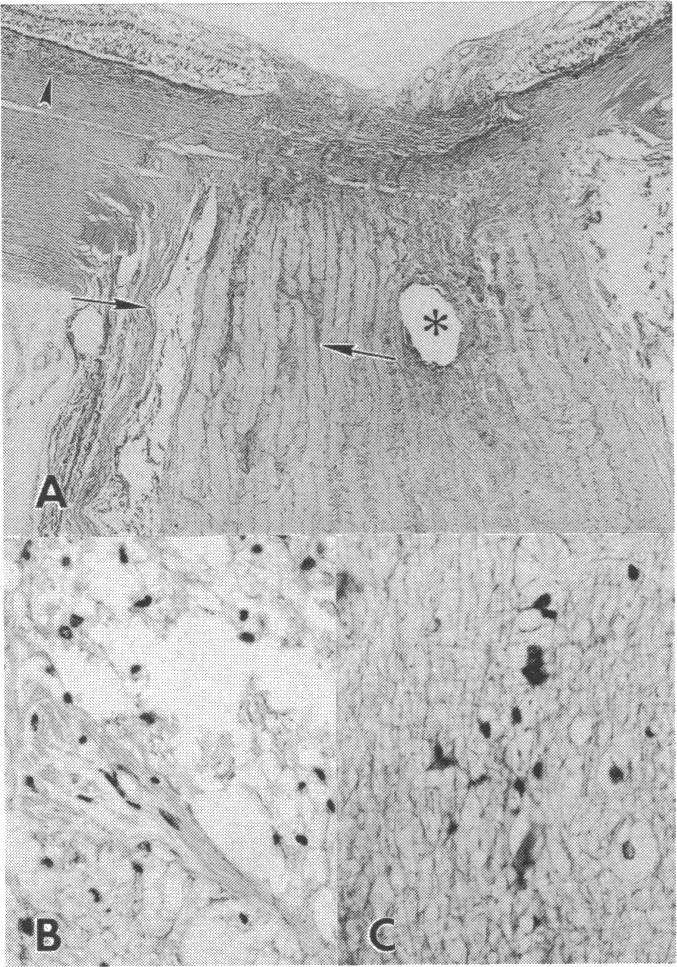
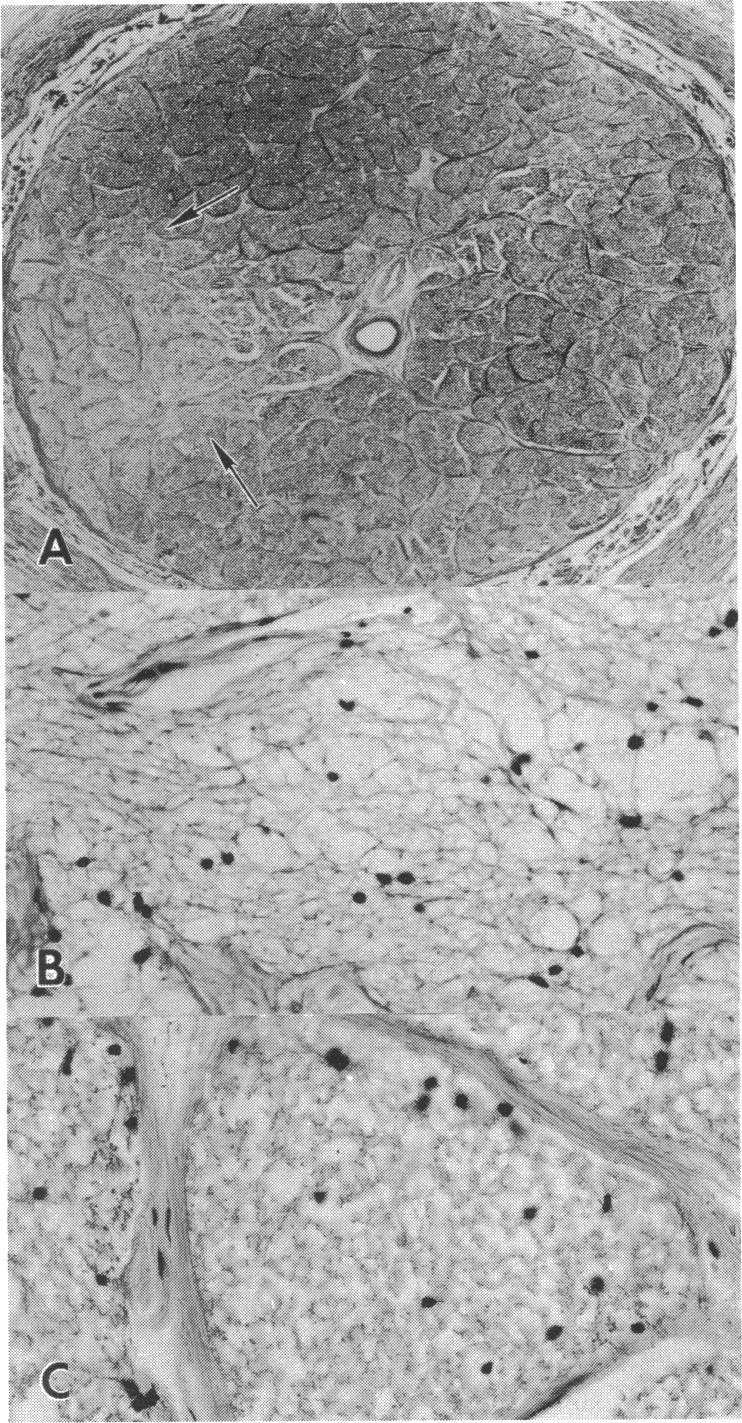
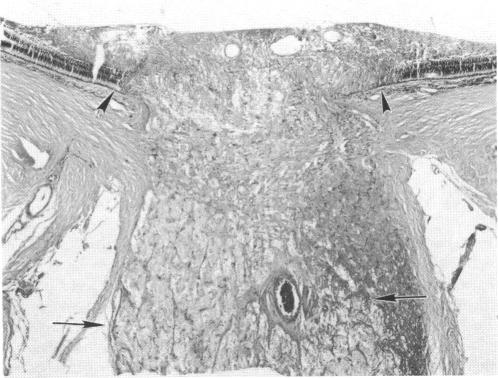
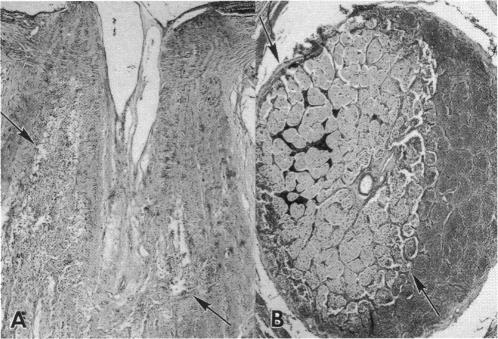
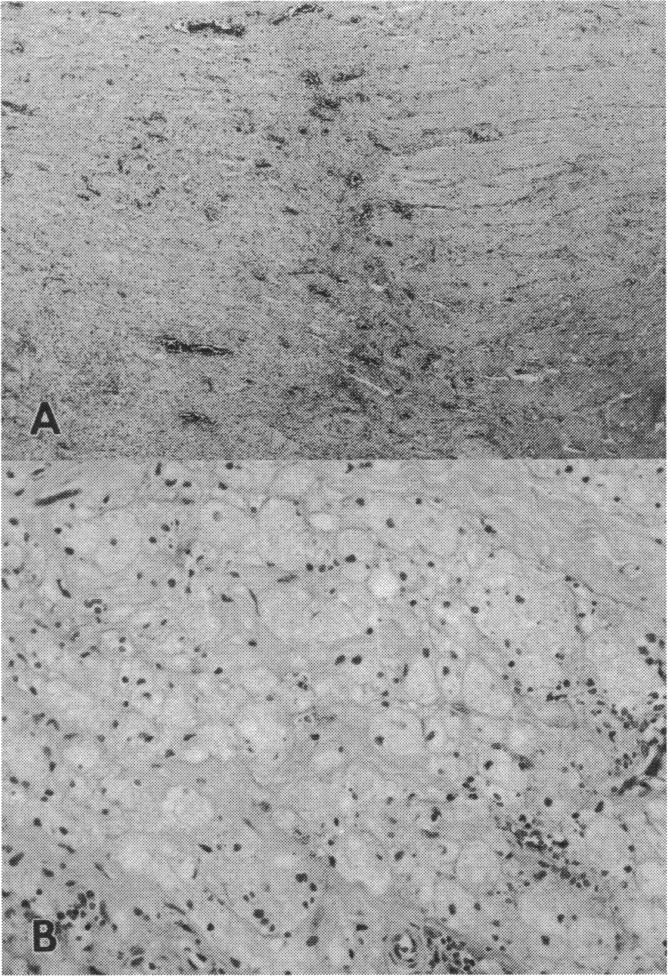
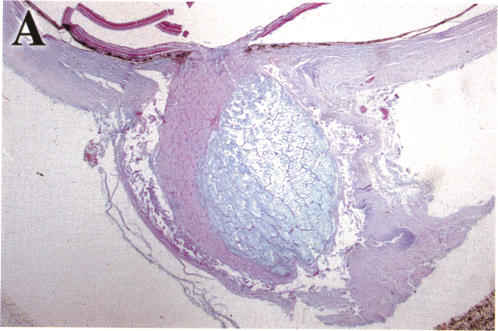
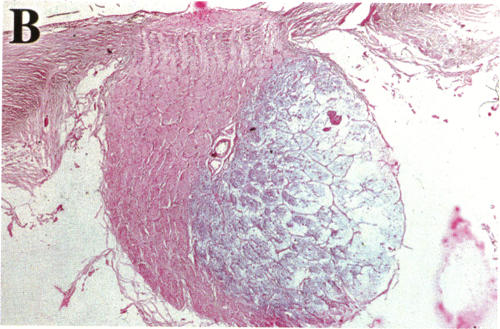
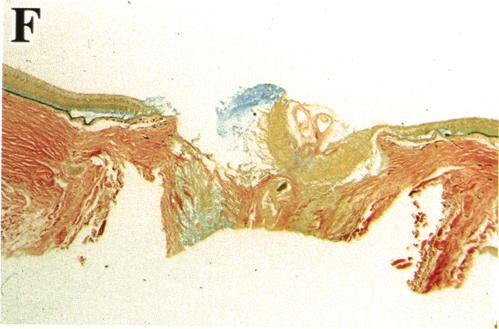
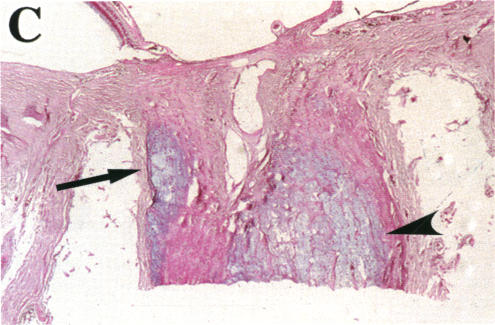
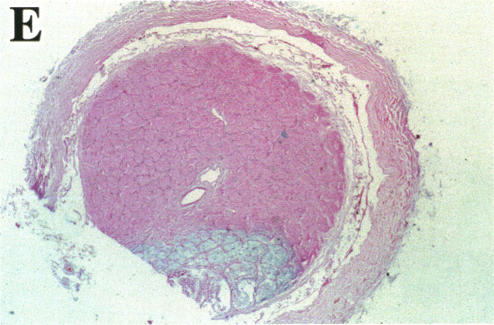
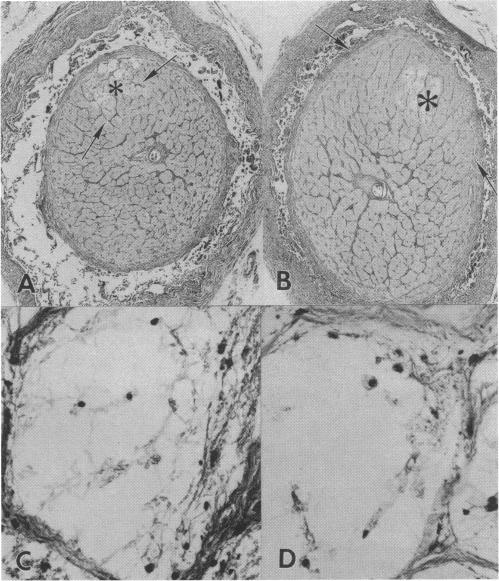
Ischemic optic neuropathy was present in 193 eyes. There were 88 females and 65 males. The average age was 71.6 years. Ischemic edema without (early) and with (later) gitter macrophages was present in 26 (13.5%). Cavernous degeneration was present in 69 nerves (36%). Mucopolysaccharide (MPS) was present in 37 cavernous lesions 1 month or longer after loss of vision. Cavernous lesions were seen in 3 eyes in which peripapillary retinal nerve fiber layer hemorrhage had been observed prior to death. Atrophic lesions, the most common pattern, were observed in 133 optic nerves (66.8%). More than 1 ischemic lesion was seen in 38 optic nerves (19.7%). Bilateral ischemic lesions were seen in 50 (35.2%) of 142 paired eyes.
Ischemic optic nerve lesions are initially acellular and later show macrophage infiltration. Cavernous lesions with MPS are present 4 weeks or longer after vision loss. The location of MPS posteriorly and along the internal margin suggests that MPS is produced at the edges of lesions. Progressive vision loss in ischemic optic neuropathy may be secondary to compression of intact nerve from ischemic edema and cavernous swelling, or a second ischemic lesion.
明确1951年至1998年间病理诊断为缺血性视神经病变的眼部组织病理学特征。
记录以下数据:患者年龄、种族、性别、组织来源、死亡原因、临床病史、视力丧失至死亡的间隔时间、眼球摘除、眶内容剜除及活检情况。缺血性视神经病变的组织病理学诊断标准为视神经局部存在缺血性水肿、海绵状变性或视神经上下方的萎缩区域。将视力突然丧失患者的病例与文献报道相结合,构建组织病理学特征及相关情况的时间表。
193只眼中存在缺血性视神经病变。其中女性88例,男性65例。平均年龄为71.6岁。无(早期)和有(后期)格子细胞巨噬细胞的缺血性水肿分别见于26只眼(13.5%)。69条神经存在海绵状变性(36%)。视力丧失1个月或更长时间后,37个海绵状病变中存在黏多糖(MPS)。在3只生前观察到视乳头周围视网膜神经纤维层出血的眼中可见海绵状病变。萎缩性病变是最常见的类型,见于133条视神经(66.8%)。38条视神经(19.7%)中可见不止1个缺血性病变。142对双眼中有50对(35.2%)出现双侧缺血性病变。
缺血性视神经病变最初无细胞,随后出现巨噬细胞浸润。视力丧失4周或更长时间后出现伴有MPS的海绵状病变。MPS在病变后部及沿内侧边缘的位置提示其在病变边缘产生。缺血性视神经病变中进行性视力丧失可能继发于缺血性水肿和海绵状肿胀对完整神经的压迫,或继发于第二个缺血性病变。