Rapoport A P, Meisenberg B, Sarkodee-Adoo C, Fassas A, Frankel S R, Mookerjee B, Takebe N, Fenton R, Heyman M, Badros A, Kennedy A, Jacobs M, Hudes R, Ruehle K, Smith R, Kight L, Chambers S, MacFadden M, Cottler-Fox M, Chen T, Phillips G, Tricot G
Greenebaum Cancer Center and Stem Cell Transplantation Program, University of Maryland School of Medicine, Baltimore, MD, USA.
Bone Marrow Transplant. 2002 Feb;29(4):303-12. doi: 10.1038/sj.bmt.1703363.
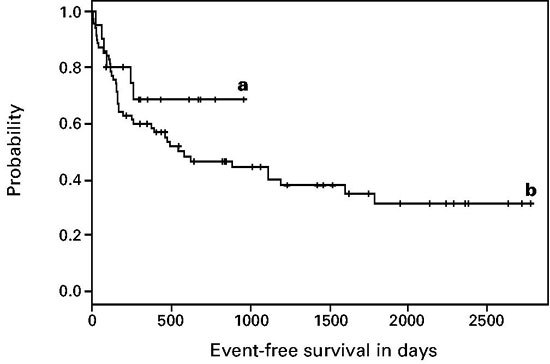
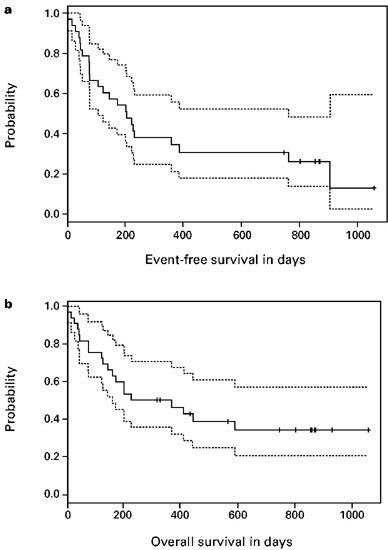
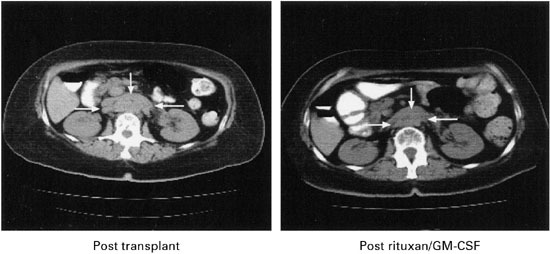
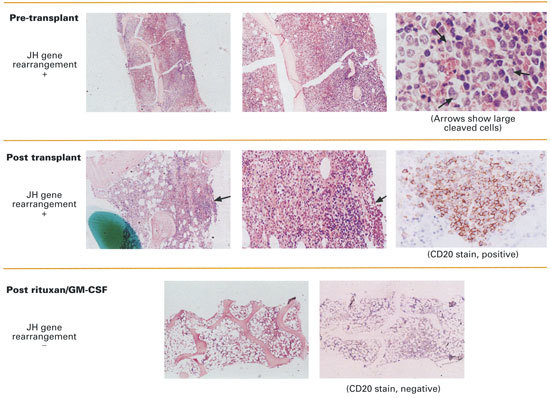
Disease relapse occurs in 50% or more of patients who are autografted for relapsed or refractory lymphoma (NHL) or Hodgkin's disease (HD). The administration of non-cross-resistant therapies during the post-transplant phase could possibly control residual disease and delay or prevent its progression. To test this approach, 55 patients with relapsed/refractory or high-risk NHL or relapsed/refractory HD were enrolled in the following protocol: stem cell mobilization: cyclophosphamide (4.5 g/m(2)) + etoposide (2.0 g/m(2)) followed by GM-CSF or G-CSF; high-dose therapy: gemcitabine (1.0 g/m(2)) on day -5, BCNU (300 mg/m(2)) + gemcitabine (1.0 g/m(2)) on day -2, melphalan (140 mg/m(2)) on day -1, blood stem cell infusion on day 0; post-transplant immunotherapy (B cell NHL): rituxan (375 mg/m(2)) weekly for 4 weeks + GM-CSF (250 microg thrice weekly) (weeks 4-8); post-transplant involved-field radiotherapy (HD): 30-40 Gy to pre-transplant areas of disease (weeks 4-8); post-transplant consolidation chemotherapy (all patients): dexamethasone (40 mg daily)/cyclophosphamide (300 mg/m(2)/day)/etoposide (30 mg/m(2)/day)/cisplatin (15 mg/m(2)/day) by continuous intravenous infusion for 4 days + gemcitabine (1.0 g/m(2), day 3) (months 3 + 9) alternating with dexamethasone/paclitaxel (135 mg/m(2))/cisplatin (75 mg/m(2)) (months 6 + 12). Of the 33 patients with B cell lymphoma, 14 had primary refractory disease (42%), 12 had relapsed disease (36%) and seven had high-risk disease in first CR (21%). For the entire group, the 2-year Kaplan-Meier event-free survival (EFS) and overall survival (OS) were 30% and 35%, respectively, while six of 33 patients (18%) died before day 100 from transplant-related complications. The rituxan/GM-CSF phase was well-tolerated by the 26 patients who were treated and led to radiographic responses in seven patients; an eighth patient with a blastic variant of mantle-cell lymphoma had clearance of marrow involvement after rituxan/GM-CSF. Of the 22 patients with relapsed/refractory HD (21 patients) or high-risk T cell lymphoblastic lymphoma (one patient), the 2-year Kaplan-Meier EFS and OS were 70% and 85%, respectively, while two of 22 patients (9%) died before day 100 from transplant-related complications. Eight patients received involved field radiation and seven had radiographic responses within the treatment fields. A total of 72 courses of post-transplant consolidation chemotherapy were administered to 26 of the 55 total patients. Transient grade 3-4 myelosuppression was common and one patient died from neutropenic sepsis, but no patients required an infusion of backup stem cells. After adjustment for known prognostic factors, the EFS for the cohort of HD patients was significantly better than the EFS for an historical cohort of HD patients autografted after BEAC (BCNU/etoposide/cytarabine/cyclophosphamide) without consolidation chemotherapy (P = 0.015). In conclusion, post-transplant consolidation therapy is feasible and well-tolerated for patients autografted for aggressive NHL and HD and may be associated with improved progression-free survival particularly for patients with HD.
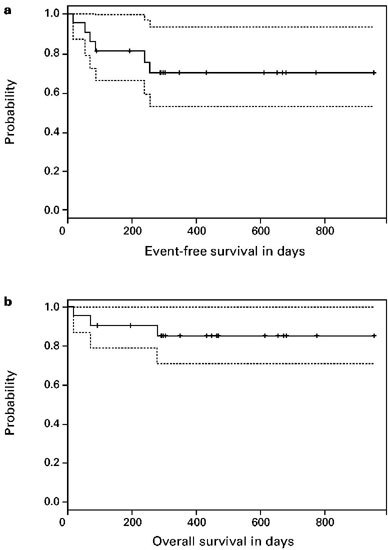
对于接受自体移植治疗复发或难治性淋巴瘤(非霍奇金淋巴瘤,NHL)或霍奇金病(HD)的患者,50%或更多会出现疾病复发。在移植后阶段给予非交叉耐药疗法可能控制残留疾病并延迟或预防其进展。为了验证这种方法,55例复发/难治性或高危NHL患者或复发/难治性HD患者入组了以下方案:干细胞动员:环磷酰胺(4.5 g/m²)+依托泊苷(2.0 g/m²),随后给予粒细胞巨噬细胞集落刺激因子(GM-CSF)或粒细胞集落刺激因子(G-CSF);大剂量治疗:第-5天给予吉西他滨(1.0 g/m²),第-2天给予卡莫司汀(BCNU,300 mg/m²)+吉西他滨(1.0 g/m²),第-1天给予美法仑(140 mg/m²),第0天进行造血干细胞输注;移植后免疫治疗(B细胞NHL):利妥昔单抗(375 mg/m²)每周1次,共4周+GM-CSF(250 μg,每周3次)(第4 - 8周);移植后受累野放疗(HD):对移植前疾病部位给予30 - 40 Gy照射(第4 - 8周);移植后巩固化疗(所有患者):地塞米松(40 mg/天)/环磷酰胺(300 mg/m²/天)/依托泊苷(30 mg/m²/天)/顺铂(15 mg/m²/天)持续静脉输注4天+吉西他滨(1.0 g/m²,第3天)(第3和9个月),与地塞米松/紫杉醇(135 mg/m²)/顺铂(75 mg/m²)交替使用(第6和12个月)。33例B细胞淋巴瘤患者中,14例为原发性难治性疾病(42%),12例为复发性疾病(36%),7例在首次完全缓解(CR)时为高危疾病(21%)。对于整个组,2年的无事件生存率(EFS)和总生存率(OS)分别为30%和35%,而33例患者中有6例(18%)在第100天前死于移植相关并发症。接受治疗的26例患者对利妥昔单抗/GM-CSF阶段耐受性良好,7例患者出现影像学缓解;1例套细胞淋巴瘤母细胞变异型患者在接受利妥昔单抗/GM-CSF治疗后骨髓受累消失。22例复发/难治性HD患者(21例)或高危T细胞淋巴母细胞淋巴瘤患者(1例)中,2年的Kaplan-Meier EFS和OS分别为70%和85%,22例患者中有2例(9%)在第100天前死于移植相关并发症。8例患者接受了受累野放疗,7例在治疗野内出现影像学缓解。55例患者中的26例共接受了72个疗程的移植后巩固化疗。短暂的3 - 4级骨髓抑制很常见,1例患者死于中性粒细胞减少性败血症,但没有患者需要输注备用干细胞。在对已知预后因素进行调整后,HD患者队列的EFS显著优于接受BEAC(卡莫司汀/依托泊苷/阿糖胞苷/环磷酰胺)后未进行巩固化疗的HD患者历史队列(P = 0.015)。总之,移植后巩固治疗对于接受自体移植治疗侵袭性NHL和HD的患者是可行且耐受性良好的,并且可能与无进展生存期改善相关,特别是对于HD患者。