Ulrich-Pur H, Raderer M, Verena Kornek G, Schüll B, Schmid K, Haider K, Kwasny W, Depisch D, Schneeweiss B, Lang F, Scheithauer W
Department of Internal Medicine I, University Hospital, Vienna, Australia.
Br J Cancer. 2003 Apr 22;88(8):1180-4. doi: 10.1038/sj.bjc.6600883.
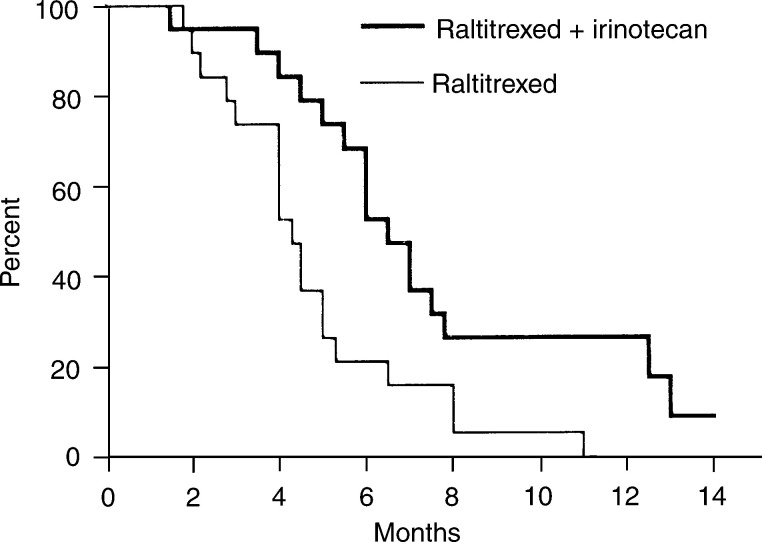
There is no established second-line treatment for advanced pancreatic cancer after gemcitabine failure. In view of the urgent need for such therapy, and since preclinical and phase I clinical data suggest an encouraging, potentially synergistic activity between raltitrexed and irinotecan, the present randomised phase II study was initiated. A total of 38 patients with metastatic pancreatic adenocarcinoma, who progressed while receiving or within 6 months after discontinuation of palliative first-line chemotherapy with gemcitabine, were enrolled in this study. They were randomised to 3-weekly courses of raltitrexed 3 mg x m(-2) on day 1 (arm A) or irinotecan 200 mg x m(-2) on day 1 plus raltitrexed 3 mg x m(-2) on day 2 (arm B). The primary study end point was objective response, secondary end points included progression-free survival (PFS) and overall survival (OS), as well as clinical benefit response in symptomatic patients (n=28). In the combination arm, the IRC-confirmed objective response rate was 16% (three out of 19 patients had a partial remission; 95% CI, 3-40%), which was clearly superior to that in the comparator/control arm with raltitrexed alone, in which no response was obtained. Therefore, the trial was already stopped at the first stage of accrual. Also, the secondary study end points, median PFS (2.5 vs 4.0 months), OS (4.3 vs 6.5 months), and clinical benefit response (8 vs 29%) were superior in the combination arm. The objective and subjective benefits of raltitrexed+irinotecan were not negated by severe, clinically relevant treatment-related toxicities: gastrointestinal symptoms (42 vs 68%), partial alopecia (0 vs 42%), and cholinergic syndrome (0 vs 21%) were more commonly noted in arm B; however, grade 3 adverse events occurred in only three patients in both treatment groups. Our data indicate that combined raltitrexed+irinotecan seems to be an effective salvage regimen in patients with gemcitabine-pretreated pancreatic cancer. The superior response activity, PFS and OS (when compared to raltitrexed), as well as its tolerability and ease of administration suggest that future trials with this combination are warranted.
对于吉西他滨治疗失败后的晚期胰腺癌,尚无既定的二线治疗方案。鉴于对此类疗法的迫切需求,且临床前和I期临床数据表明雷替曲塞与伊立替康之间存在令人鼓舞的潜在协同活性,遂开展了本项随机II期研究。本研究共纳入38例转移性胰腺腺癌患者,这些患者在接受吉西他滨姑息一线化疗期间或停药后6个月内病情进展。他们被随机分为两组,分别接受为期3周的治疗:A组在第1天给予雷替曲塞3 mg/m²;B组在第1天给予伊立替康200 mg/m²,在第2天给予雷替曲塞3 mg/m²。主要研究终点为客观缓解,次要终点包括无进展生存期(PFS)和总生存期(OS),以及有症状患者(n = 28)的临床获益反应。在联合治疗组中,经独立审查委员会(IRC)确认的客观缓解率为16%(19例患者中有3例部分缓解;95%CI,3 - 40%),明显优于单独使用雷替曲塞的对照/比较组,该组未观察到缓解。因此,该试验在入组的第一阶段就已停止。此外,联合治疗组的次要研究终点,中位PFS(2.5个月对4.0个月)、OS(4.3个月对6.5个月)和临床获益反应(8%对29%)也更优。雷替曲塞 + 伊立替康的客观和主观获益并未被严重的、临床相关的治疗相关毒性所抵消:B组更常出现胃肠道症状(42%对68%)、部分脱发(0%对42%)和胆碱能综合征(0%对21%);然而,两个治疗组中均仅有3例患者发生3级不良事件。我们的数据表明,雷替曲塞 + 伊立替康联合方案似乎是吉西他滨预处理的胰腺癌患者有效的挽救治疗方案。与雷替曲塞相比,其具有更好的缓解活性、PFS和OS,以及耐受性和给药便利性,提示有必要开展该联合方案的后续试验。