Ruo Bernice, Rumsfeld John S, Hlatky Mark A, Liu Haiying, Browner Warren S, Whooley Mary A
Section of General Internal Medicine, Veterans Affairs Medical Center, San Francisco 94121, USA.
JAMA. 2003 Jul 9;290(2):215-21. doi: 10.1001/jama.290.2.215.
Little is known regarding the extent to which patient-reported health status, including symptom burden, physical limitation, and quality of life, is determined by psychosocial vs physiological factors among patients with chronic disease.
To compare the contributions of depressive symptoms and measures of cardiac function to the health status of patients with coronary artery disease.
DESIGN, SETTING, AND PARTICIPANTS: Cross-sectional study of 1024 adults with stable coronary artery disease recruited from outpatient clinics in the San Francisco Bay Area between September 2000 and December 2002. Main Measures Measurement of depressive symptoms using the Patient Health Questionnaire (PHQ); assessment of cardiac function by measuring left ventricular ejection fraction on echocardiography, exercise capacity on treadmill testing, and ischemia on stress echocardiography; and measurement of a range of health status outcomes, including symptom burden, physical limitation, and quality of life, using the Seattle Angina Questionnaire. Participants were also asked to rate their overall health as excellent, very good, good, fair, or poor.
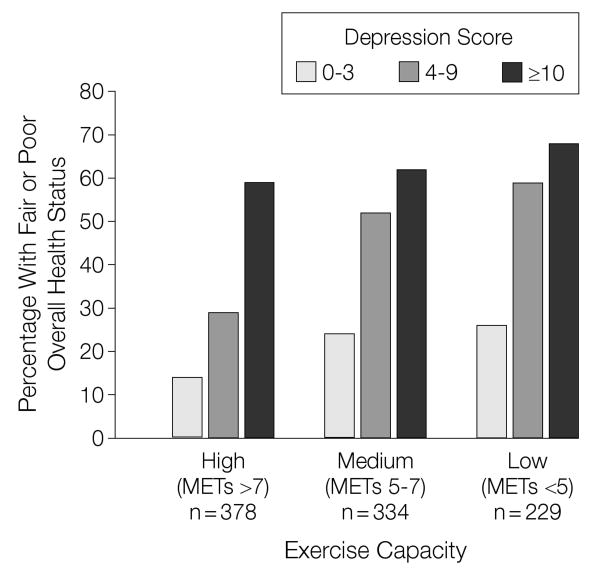
Of the 1024 participants, 201 (20%) had depressive symptoms (PHQ score > or =10). Participants with depressive symptoms were more likely than those without depressive symptoms to report at least mild symptom burden (60% vs 33%; P<.001), mild physical limitation (73% vs 40%; P<.001), mildly diminished quality of life (67% vs 31%; P<.001), and fair or poor overall health (66% vs 30%; P<.001). In multivariate analyses adjusting for measures of cardiac function and other patient characteristics, depressive symptoms were strongly associated with greater symptom burden (odds ratio [OR], 1.8; 95% confidence interval [CI], 1.3-2.7; P =.002), greater physical limitation (OR, 3.1; 95% CI, 2.1-4.6; P<.001), worse quality of life (OR, 3.1; 95% CI, 2.2-4.6; P<.001), and worse overall health (OR, 2.0; 95% CI, 1.3-2.9; P<.001). Although decreased exercise capacity was associated with worse health status, left ventricular ejection fraction and ischemia were not.
Among patients with coronary disease, depressive symptoms are strongly associated with patient-reported health status, including symptom burden, physical limitation, quality of life, and overall health. Conversely, 2 traditional measures of cardiac function-ejection fraction and ischemia-are not. Efforts to improve health status should include assessment and treatment of depressive symptoms.
关于慢性病患者报告的健康状况(包括症状负担、身体限制和生活质量)在多大程度上由心理社会因素而非生理因素决定,目前所知甚少。
比较抑郁症状和心功能指标对冠状动脉疾病患者健康状况的影响。
设计、地点和参与者:2000年9月至2002年12月期间从旧金山湾区门诊招募的1024例稳定型冠状动脉疾病成年患者的横断面研究。主要测量方法 使用患者健康问卷(PHQ)测量抑郁症状;通过超声心动图测量左心室射血分数、跑步机测试评估运动能力以及负荷超声心动图评估缺血情况来评估心功能;使用西雅图心绞痛问卷测量一系列健康状况结果,包括症状负担、身体限制和生活质量。参与者还被要求将他们的总体健康状况评为优秀、非常好、好、一般或差。
在1024名参与者中,201名(20%)有抑郁症状(PHQ评分≥10)。有抑郁症状的参与者比没有抑郁症状的参与者更有可能报告至少轻度的症状负担(60%对33%;P<0.001)、轻度身体限制(73%对40%;P<0.001)、生活质量轻度下降(67%对31%;P<0.001)以及总体健康状况为一般或差(66%对30%;P<0.001)。在对心功能指标和其他患者特征进行调整的多变量分析中,抑郁症状与更大的症状负担(优势比[OR],1.8;95%置信区间[CI],1.3 - 2.7;P = 0.002)、更大的身体限制(OR,3.1;95%CI,2.1 - 4.6;P<0.001)、更差的生活质量(OR,3.1;95%CI,2.2 - 4.6;P<0.001)以及更差的总体健康状况(OR,2.0;95%CI,1.3 - 2.9;P<0.001)密切相关。虽然运动能力下降与更差的健康状况相关,但左心室射血分数和缺血情况并非如此。
在冠心病患者中,抑郁症状与患者报告的健康状况密切相关,包括症状负担、身体限制、生活质量和总体健康状况。相反,两种传统的心功能测量指标——射血分数和缺血情况——并非如此。改善健康状况的努力应包括对抑郁症状的评估和治疗。