Salameh Jihad R, Salloum Ellis J
University of Mississippi Medical Center, Jackson, Mississippi 39216, USA.
JSLS. 2004 Oct-Dec;8(4):391-4.
Lumbar hernias occur infrequently and can be congenital, primary (inferior or Petit type, and superior or Grynfeltt type), posttraumatic, or incisional. They are bounded by the 12th rib, the iliac crest, the erector spinae, and the external oblique muscle. Most postoperative incisional hernias occur in nephrectomy or aortic aneurysm repair incisions.
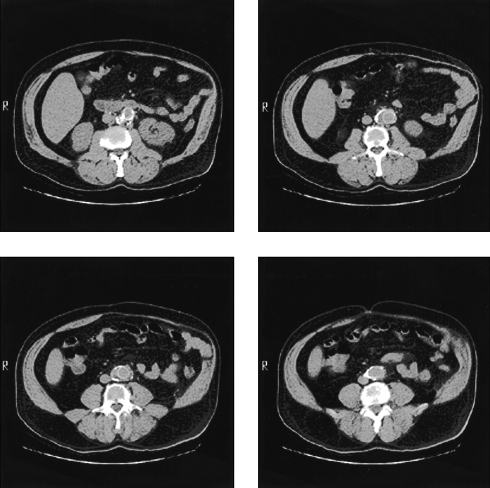
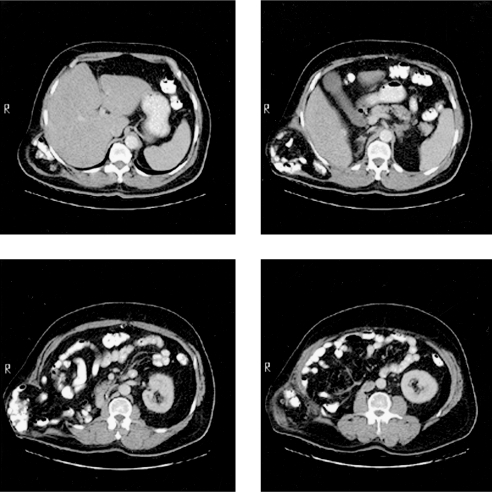
We present 2 patients who had undergone flank incisions and subsequently developed significant bulging of that area. The first patient had an atrophy of the abdominal wall musculature while the other had a large lumbar incisional hernia that was repaired laparoscopically.
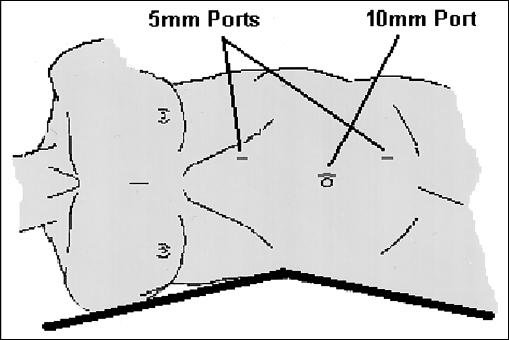
Lumbar incisional hernias are often diffuse with fascial defects that are usually hard to appreciate. Computed tomography scan is the diagnostic modality of choice and allows differentiating them from abdominal wall musculature denervation atrophy complicating flank incisions. Repairing these hernias is difficult due to the surrounding structures. Principles of laparoscopic repair include lateral decubitus positioning with table flexed, adhesiolysis, and reduction of hernia contents, securing ePTFE mesh with spiral tacks and transfascial sutures to an intercostal space superiorly, iliac crest periosteum inferiorly, and rectus muscle anteriorly. Posteriorly, the mesh is secured to psoas major fascia with intracorporeal sutures to avoid nerve injury.
Lumbar incisional hernia must be differentiated from muscle atrophy with no fascial defect. The laparoscopic approach provides an attractive option for this often challenging problem.
腰椎疝并不常见,可分为先天性、原发性(下位或佩蒂型,以及上位或格林费尔特型)、创伤后或切口疝。它们由第12肋、髂嵴、竖脊肌和腹外斜肌所界定。大多数术后切口疝发生在肾切除术或主动脉瘤修复切口处。
我们介绍2例接受过侧腹切口手术且随后该区域出现明显隆起的患者。第一例患者腹壁肌肉组织萎缩,另一例患者有一个大型腰椎切口疝,通过腹腔镜进行了修复。
腰椎切口疝通常较为弥漫,伴有筋膜缺损,往往难以察觉。计算机断层扫描是首选的诊断方法,可将其与侧腹切口并发的腹壁肌肉组织去神经萎缩相鉴别。由于周围结构的原因,修复这些疝很困难。腹腔镜修复的原则包括侧卧位并使手术台弯曲、松解粘连、还纳疝内容物,用螺旋钉和经筋膜缝线将ePTFE补片固定于上方的肋间间隙、下方的髂嵴骨膜和前方的腹直肌。在后方,用体内缝线将补片固定于腰大肌筋膜,以避免神经损伤。
腰椎切口疝必须与无筋膜缺损的肌肉萎缩相鉴别。腹腔镜手术方法为这个常常具有挑战性的问题提供了一个有吸引力的选择。