Swindells Susan, Cohen Calvin J, Berger Daniel S, Tashima Karen T, Liao Qiming, Pobiner Bonnie F, Snidow Jerry W, Pakes Gary E, Hernandez Jaime E
HIV Clinic, University of Nebraska Medical Center, Omaha, NE, USA.
BMC Infect Dis. 2005 Apr 8;5:23. doi: 10.1186/1471-2334-5-23.
Hydroxyurea (HU) is an immunomodulatory agent that has been documented to enhance the antiretroviral activity of nucleoside reverse transcriptase inhibitors, such as abacavir (ABC) and didanosine (ddI), and would be expected to improve virologic efficacy.
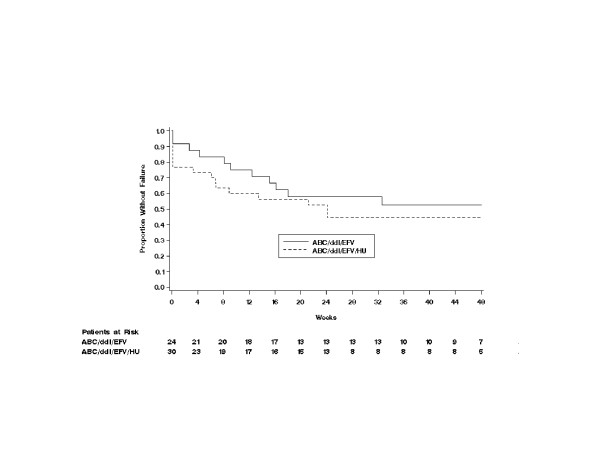
A 48-week, phase IV, multicenter, open-label, proof-of-concept clinical trial was conducted to evaluate second-line, protease inhibitor (PI)-sparing therapy with ABC/efavirenz (EFV)/ddI plus HU or without HU in HIV-infected subjects failing to achieve HIV-1 RNA < or = 400 copies/mL after > or = 16 weeks of treatment with lamivudine/zidovudine or lamivudine/stavudine, plus 1 or 2 PIs. Subjects were assigned to ABC (300 mg twice daily)/ EFV (600 mg once daily)/ ddI (400 mg once daily) plus HU (500 mg twice daily) (n = 30) or this regimen without HU (n = 24).
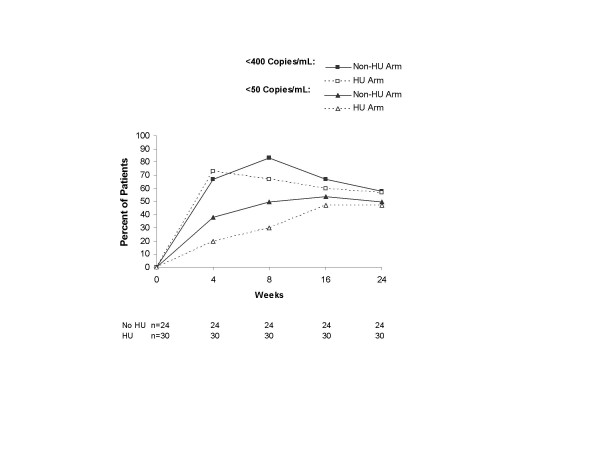
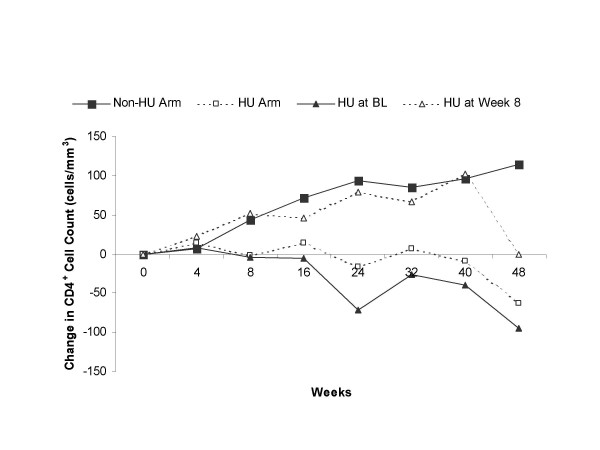
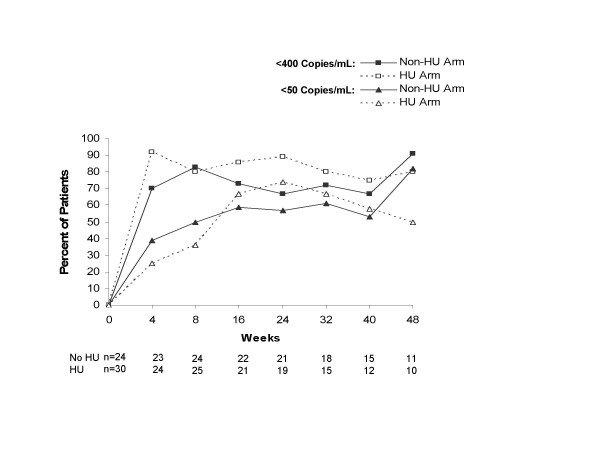
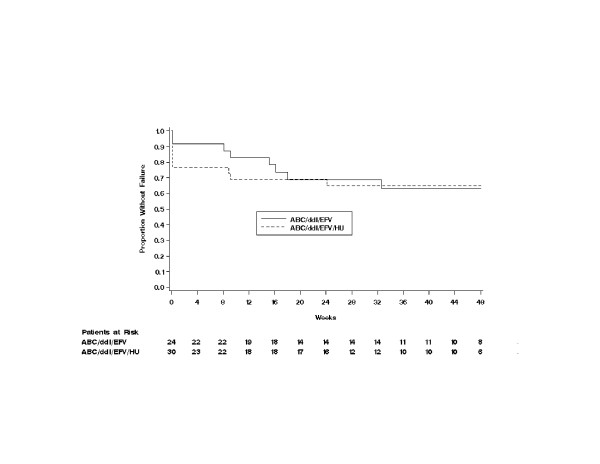
Baseline mean HIV-1 RNA was 3.86 log10 copies/mL and CD4+ cell count was 345 cells/mm3. A similar percentage of subjects in the non-HU arm (58%) and HU arm (53%) completed the study. Intent-to-treat: missing = failure analysis showed no differences in proportions of subjects in the non-HU and HU arms achieving undetectable plasma HIV-1 RNA levels at week 24 (< 400 copies/mL: 58% [14/24] vs 57% [17/30], P = 0.899; < 50 copies/mL (50% [12/24] vs 47% [14/30], P = 0.780). Median change from baseline in CD4+ cell count in the non-HU and HU arms at week 48 was +114 cells/mm3 and -63 cells/mm3 (P = 0.007), respectively. Both regimens were generally well tolerated, although more subjects in the HU arm withdrew prematurely from the study due to adverse events (23% vs 4%). Four cases of possible ABC-related hypersensitivity were observed.
ABC/EFV/ddI was an effective and well-tolerated second-line regimen for nucleoside/PI-experienced HIV-infected subjects. The addition of HU blunted the CD4+ cell response, did not appear to enhance antiviral activity, and resulted in more treatment-limiting adverse events.
羟基脲(HU)是一种免疫调节剂,已被证明可增强核苷类逆转录酶抑制剂(如阿巴卡韦(ABC)和去羟肌苷(ddI))的抗逆转录病毒活性,预计可提高病毒学疗效。
进行了一项为期48周的IV期多中心开放标签概念验证临床试验,以评估在接受拉米夫定/齐多夫定或拉米夫定/司他夫定加1或2种蛋白酶抑制剂(PI)治疗≥16周后未实现HIV-1 RNA≤400拷贝/mL的HIV感染受试者中,使用ABC/依非韦伦(EFV)/ddI加HU或不加HU的二线、不使用PI的治疗方案。受试者被分配至ABC(每日两次,每次300mg)/EFV(每日一次,600mg)/ddI(每日一次,400mg)加HU(每日两次,每次500mg)组(n = 30)或不使用HU的该方案组(n = 24)。
基线时HIV-1 RNA平均为3.86 log10拷贝/mL,CD4 +细胞计数为345个细胞/mm³。非HU组(58%)和HU组(53%)完成研究的受试者比例相似。意向性分析:缺失=失败分析显示,非HU组和HU组在第24周达到血浆HIV-1 RNA水平不可检测(<400拷贝/mL:58%[14/24]对57%[17/30],P = 0.899;<50拷贝/mL:50%[12/24]对47%[14/30],P = 0.780)的受试者比例无差异。非HU组和HU组在第48周时CD4 +细胞计数相对于基线的中位数变化分别为+114个细胞/mm³和 - 63个细胞/mm³(P = 0.007)。两种方案总体耐受性良好,尽管HU组有更多受试者因不良事件提前退出研究(23%对4%)。观察到4例可能与ABC相关的超敏反应。
ABC/EFV/ddI是核苷类/PI经治的HIV感染受试者有效的且耐受性良好的二线方案。添加HU会减弱CD4 +细胞反应,似乎不会增强抗病毒活性,且会导致更多限制治疗的不良事件。