Sebag-Montefiore D, Glynne-Jones R, Falk S, Meadows H M, Maughan T
Cookridge Hospital, Hospital Lane, Cookridge, West Yorkshire LS16 6QB, UK.
Br J Cancer. 2005 Oct 31;93(9):993-8. doi: 10.1038/sj.bjc.6602818.
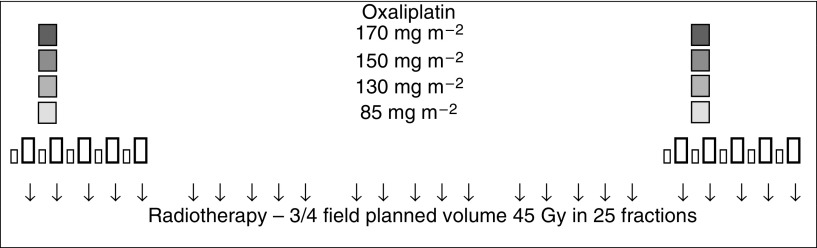
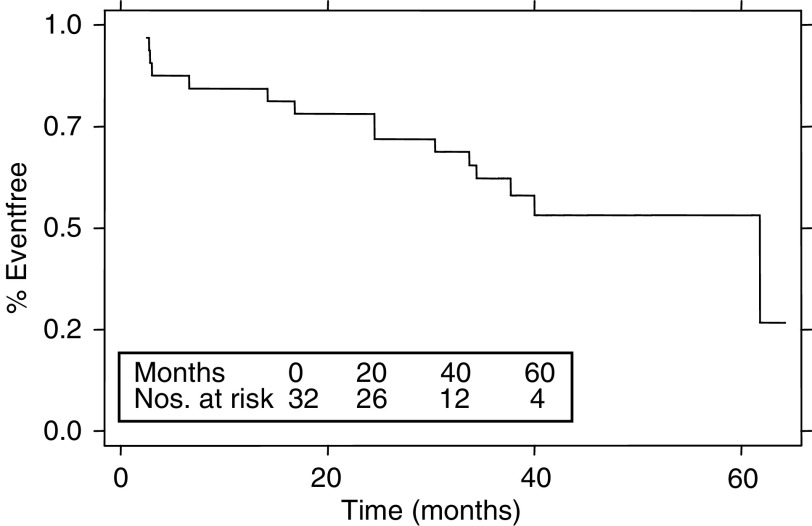
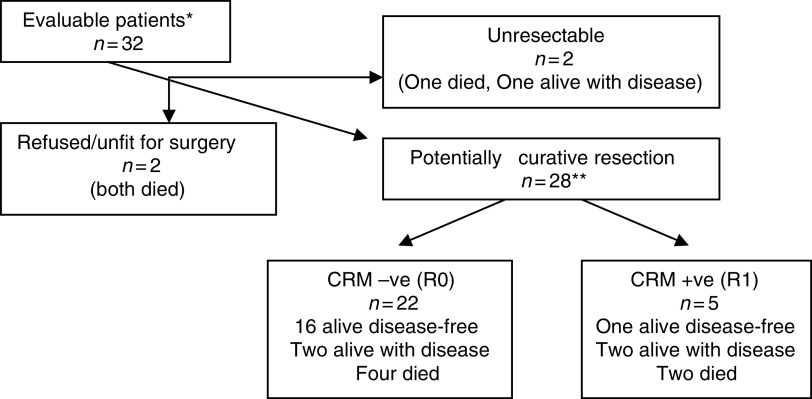
The purpose of this study was to evaluate the maximum tolerated dose (MTD) and recommended dose of oxaliplatin given synchronously with 5-fluorouracil (5FU), leucovorin (LV) and preoperative pelvic radiation for primary unresectable, locally advanced, rectal cancer. Preoperative pelvic radiotherapy using a three- or four-field technique and megavoltage photons comprised 45 Gy given in 25 fractions, 1.8 Gy per fraction, and delivered with escalating doses of oxaliplatin in combination with low-dose LV and 5FU. Chemotherapy was given synchronously with radiotherapy in weeks 1 and 5. Escalating doses of oxaliplatin (85, 130 and 150 mg m(-2)) were given on days 2 and 30, followed by low-dose LV (20 mg m(-2)) and 5FU (350 mg m(-2)), both given on days 1-5 and 29-33. Surgery was performed 6-10 weeks later. The MTD was determined as the dose causing more than a third of patients to have a dose-limiting toxicity (DLT). Once the MTD was reached, a further 14 patients were treated at the dose level below the MTD. In all, 32 patients received oxaliplatin at the three dose levels, median age 60 years (range 31-79), 24 males and eight females. The MTD was reached at 150 mg m(-2) when four out of six patients experienced DLT. Dose-limiting grade 3 or 4 diarrhoea was reported in two out of six patients at 85 mg m(-2), 5 out of 20 at 130 mg m(-2) and four out of 6 at 150 mg m(-2). Grade 3 neuropathy was reported at 130 mg m(-2) (1 out of 20) and at 150 mg m(-2) (two out of six), and serious haematological toxicity was minimal; one grade 3 anaemia at 150 mg m(-2). In all, 28 out of 32 patients completed all treatments as planned; three had radiotherapy interrupted and three a chemotherapy dose reduction. Four patients did not proceed to surgery due to the presence of metastatic disease (two), unfitness (one) or patient refusal (one). Also, 28 patients underwent surgical resection. Histopathology demonstrated histopathological complete response (pCR) 2 out of 27 (7%), Tmic 3 out of 27 (11%), pCR+Tmic 5 out of 27 (19%), pT0-2 6 out of 27 (22%) and histologically confirmed clear circumferential resection margins in 22 out of 27 (81%). Dose-limiting toxicity with oxaliplatin is 150 mg m(-2) given days 2 and 30 when added to the described 5FU LV and 45 Gy radiation preoperatively. The acceptable toxicity and compliance at 130 mg m(-2) recommend testing this dose in future phase II studies. The tumour downstaging and complete resection rates are encouragingly high for this very locally advanced group.
本研究的目的是评估奥沙利铂与5-氟尿嘧啶(5FU)、亚叶酸钙(LV)同步给药以及术前盆腔放疗用于原发性不可切除、局部晚期直肠癌的最大耐受剂量(MTD)和推荐剂量。采用三野或四野技术及兆伏光子进行术前盆腔放疗,总剂量45 Gy,分25次给予,每次1.8 Gy,并联合递增剂量的奥沙利铂、低剂量LV和5FU。化疗在第1周和第5周与放疗同步进行。在第2天和第30天给予递增剂量的奥沙利铂(85、130和150 mg m⁻²),随后在第1 - 5天和第29 - 33天给予低剂量LV(20 mg m⁻²)和5FU(350 mg m⁻²)。6 - 10周后进行手术。MTD被确定为导致超过三分之一患者出现剂量限制性毒性(DLT)的剂量。一旦达到MTD,另外14名患者在低于MTD的剂量水平接受治疗。共有32名患者在三个剂量水平接受奥沙利铂治疗,中位年龄60岁(范围31 - 79岁),男性24名,女性8名。当6名患者中有4名出现DLT时,150 mg m⁻²达到了MTD。在85 mg m⁻²时,6名患者中有2名出现3级或4级剂量限制性腹泻;在130 mg m⁻²时,20名患者中有5名出现;在150 mg m⁻²时,6名患者中有4名出现。在130 mg m⁻²(20名患者中有1名)和150 mg m⁻²(6名患者中有2名)时报告有3级神经病变,严重血液学毒性极小;在150 mg m⁻²时有1例3级贫血。32名患者中共有28名按计划完成了所有治疗;3名患者放疗中断,3名患者化疗剂量减少。4名患者由于存在转移性疾病(2名)、身体状况不佳(1名)或患者拒绝(1名)未进行手术。此外,28名患者接受了手术切除。组织病理学显示,27名患者中有2名(7%)达到组织病理学完全缓解(pCR),27名患者中有3名(11%)达到Tmic,27名患者中有5名(19%)达到pCR + Tmic,27名患者中有6名(22%)达到pT0 - 2,27名患者中有22名(81%)组织学证实切缘阴性。当在术前联合上述5FU、LV和45 Gy放疗时,奥沙利铂的剂量限制性毒性为第2天和第30天给予150 mg m⁻²。130 mg m⁻²时可接受的毒性和依从性推荐在未来的II期研究中测试该剂量。对于这个非常局部晚期的组,肿瘤降期和完全切除率高得令人鼓舞。