Mariat Christophe, Venet Christophe, Jehl François, Mwewa Sandrine, Lazarevic Vesna, Diconne Eric, Fonsale Nathalie, Carricajo Anne, Guyomarc'h Stéphane, Vermesch Régine, Aubert Gérald, Bidault Roselyne, Bertrand Jean-Claude, Zeni Fabrice
Service de Néphrologie, Hôpital Nord, CHU de Saint-Etienne, Saint-Etienne, France.
Crit Care. 2006 Feb;10(1):R26. doi: 10.1186/cc3993.
In seriously infected patients with acute renal failure and who require continuous renal replacement therapy, data on continuous infusion of ceftazidime are lacking. Here we analyzed the pharmacokinetics of ceftazidime administered by continuous infusion in critically ill patients during continuous venovenous haemodiafiltration (CVVHDF) in order to identify the optimal dosage in this setting.
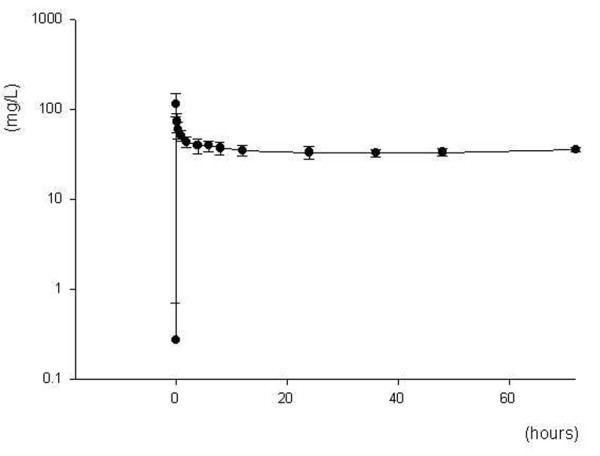
Seven critically ill patients were prospectively enrolled in the study. CVVHDF was performed using a 0.6 m2 AN69 high-flux membrane and with blood, dialysate and ultrafiltration flow rates of 150 ml/min, 1 l/hour and 1.5 l/hour, respectively. Based on a predicted haemodiafiltration clearance of 32.5 ml/min, all patients received a 2 g loading dose of ceftazidime, followed by a 3 g/day continuous infusion for 72 hours. Serum samples were collected at 0, 3, 15 and 30 minutes and at 1, 2, 4, 6, 8, 12, 24, 36, 48 and 72 hours; dialysate/ultrafiltrate samples were taken at 2, 8, 12, 24, 36 and 48 hours. Ceftazidime concentrations in serum and dialysate/ultrafiltrate were measured using high-performance liquid chromatography.
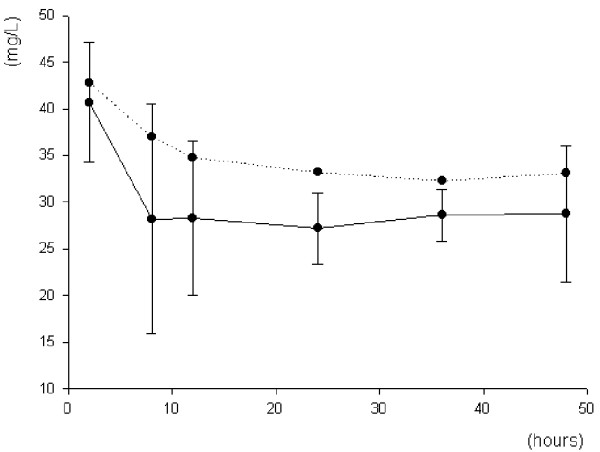
The mean (+/- standard deviation) elimination half-life, volume of distribution, area under the concentration-time curve from time 0 to 72 hours, and total clearance of ceftazidime were 4 +/- 1 hours, 19 +/- 6 l, 2514 +/- 212 mg/h per l, and 62 +/- 5 ml/min, respectively. The mean serum ceftazidime steady-state concentration was 33.5 mg/l (range 28.8-36.3 mg/l). CVVHDF effectively removed continuously infused ceftazidime, with a sieving coefficient and haemodiafiltration clearance of 0.81 +/- 0.11 and 33.6 +/- 4 mg/l, respectively.
We conclude that a dosing regimen of 3 g/day ceftazidime, by continuous infusion, following a 2 g loading dose, results in serum concentrations more than four times the minimum inhibitory concentration for all susceptible pathogens, and we recommend this regimen in critically ill patients undergoing CVVHDF.
在患有急性肾衰竭且需要持续肾脏替代治疗的重症感染患者中,缺乏关于持续输注头孢他啶的数据。在此,我们分析了在持续静静脉血液透析滤过(CVVHDF)期间重症患者持续输注头孢他啶的药代动力学,以确定在此情况下的最佳剂量。
七名重症患者前瞻性纳入本研究。使用0.6平方米的AN69高通量膜进行CVVHDF,血液、透析液和超滤流速分别为150毫升/分钟、1升/小时和1.5升/小时。基于预测的血液透析滤过清除率为32.5毫升/分钟,所有患者均接受2克头孢他啶负荷剂量,随后以3克/天持续输注72小时。在0、3、15和30分钟以及1、2、4、6、8、12、24、36、48和72小时采集血清样本;在2、8、12、24、36和48小时采集透析液/超滤液样本。使用高效液相色谱法测定血清和透析液/超滤液中头孢他啶的浓度。
头孢他啶的平均(±标准差)消除半衰期、分布容积、0至72小时浓度-时间曲线下面积和总清除率分别为4±1小时、19±6升、2514±212毫克/小时·升和62±5毫升/分钟。平均血清头孢他啶稳态浓度为33.5毫克/升(范围28.8 - 36.3毫克/升)。CVVHDF有效清除持续输注的头孢他啶,筛过系数和血液透析滤过清除率分别为0.81±0.11和33.6±4毫克/升。
我们得出结论,在2克负荷剂量后,以3克/天持续输注头孢他啶的给药方案可使血清浓度超过所有敏感病原体最低抑菌浓度的四倍以上,我们建议在接受CVVHDF的重症患者中采用该方案。