Winck João C, Azevedo Luís F, Costa-Pereira Altamiro, Antonelli Massimo, Wyatt Jeremy C
Department of Pulmonology, Faculty of Medicine, University of Porto, Portugal.
Crit Care. 2006;10(2):R69. doi: 10.1186/cc4905.
Continuous positive airway pressure ventilation (CPAP) and non-invasive positive pressure ventilation (NPPV) are accepted treatments in acute cardiogenic pulmonary edema (ACPE). However, it remains unclear whether NPPV is better than CPAP in reducing the need for endotracheal intubation (NETI) rates, mortality and other adverse events. Our aim was to review the evidence about the efficacy and safety of these two methods in ACPE management.
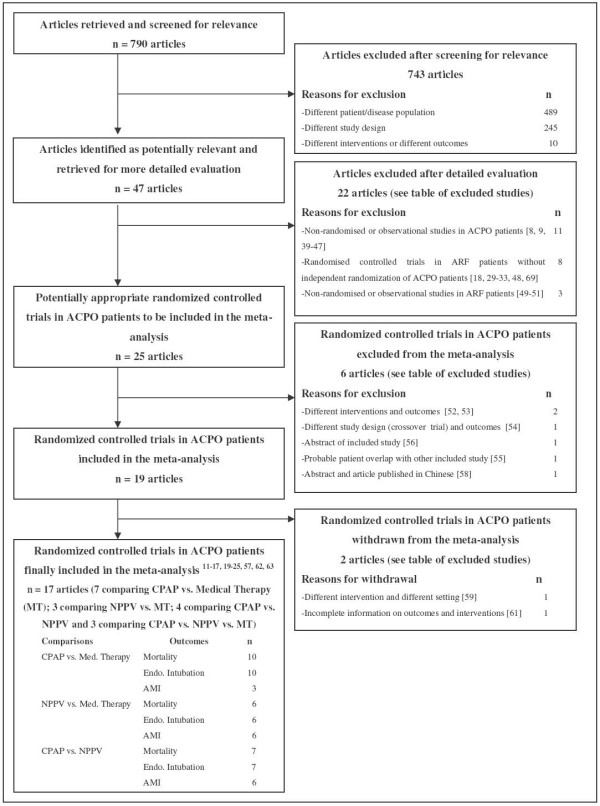
We conducted a systematic review and meta-analysis of randomized controlled trials on the effect of CPAP and/or NIPV in the treatment of ACPE, considering the outcomes NETI, mortality and incidence of acute myocardial infarction (AMI). We searched six electronic databases up to May 2005 without language restrictions, reviewed references of relevant articles, hand searched conference proceedings and contacted experts.
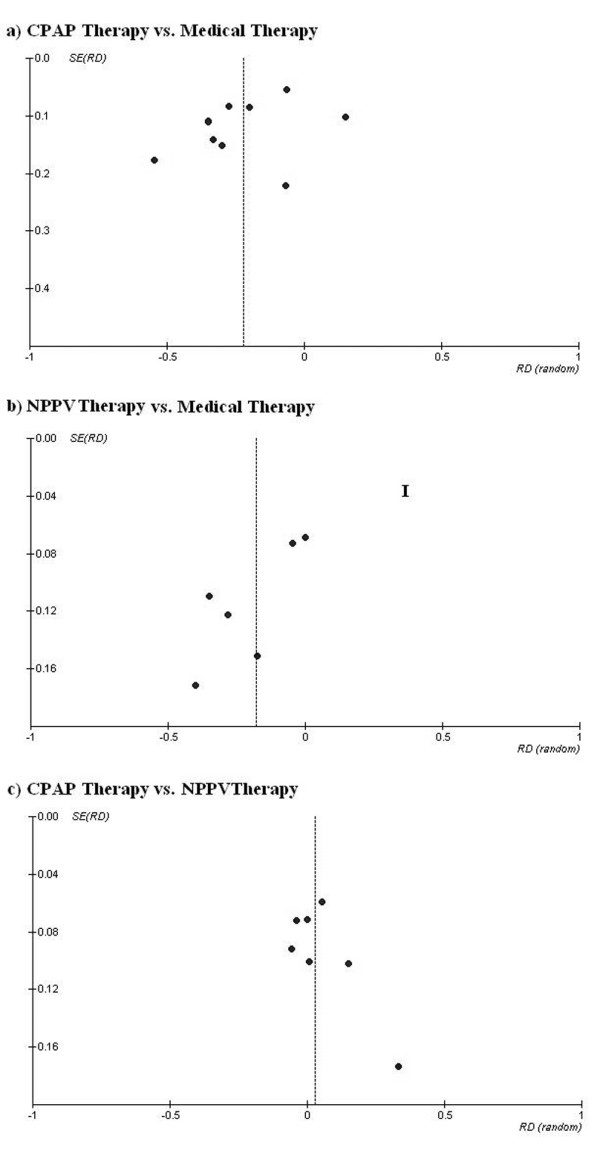
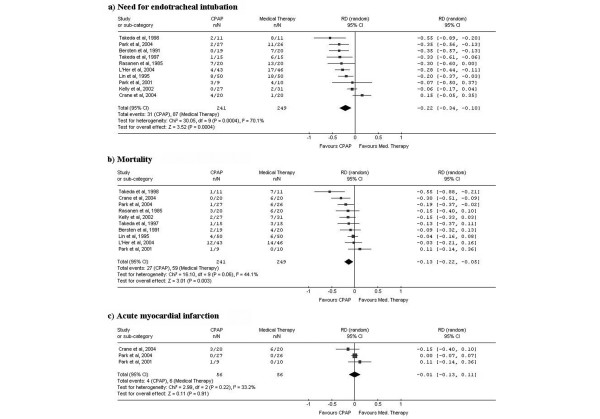
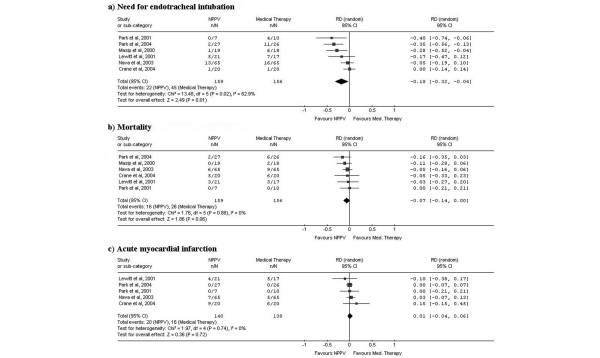
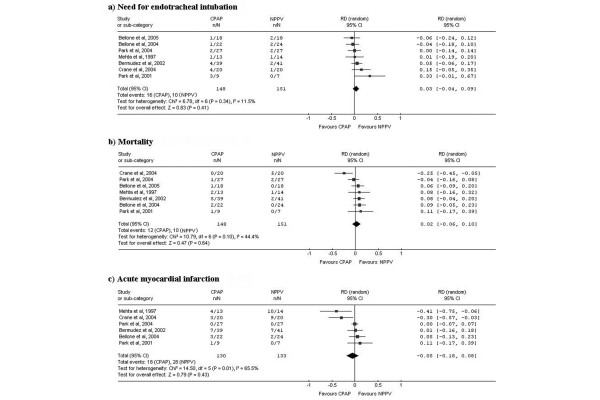
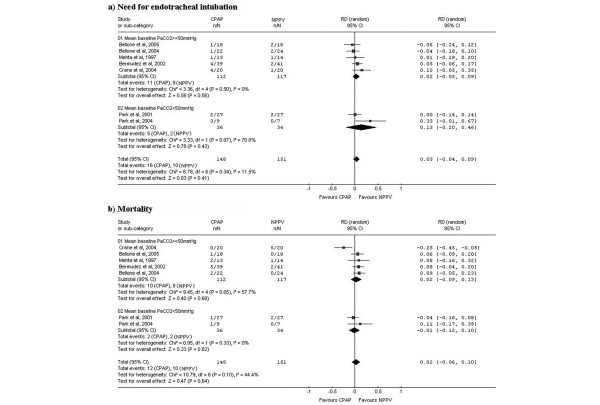
Of 790 articles identified, 17 were included. In a pooled analysis, 10 studies of CPAP compared to standard medical therapy (SMT) showed a significant 22% absolute risk reduction (ARR) in NETI (95% confidence interval (CI), -34% to -10%) and 13% in mortality (95%CI, -22% to -5%). Six studies of NPPV compared to SMT showed an 18% ARR in NETI (95%CI, -32% to -4%) and 7% in mortality (95%CI, -14% to 0%). Seven studies of NPPV compared to CPAP showed a non-significant 3% ARR in NETI (95%CI, -4% to 9%) and 2% in mortality (95%CI, -6% to 10%). None of these methods increased AMI risk. In a subgroup analysis, NPPV did not lead to better outcomes than CPAP in studies including more hypercapnic patients.
Robust evidence now supports the use of CPAP and NPPV in ACPE. Both techniques decrease NETI and mortality compared to SMT and none shows increased AMI risk. CPAP should be considered a first line intervention as NPPV did not show a better efficacy, even in patients with more severe conditions, and CPAP is cheaper and easier to implement in clinical practice.
持续气道正压通气(CPAP)和无创正压通气(NPPV)是治疗急性心源性肺水肿(ACPE)的公认方法。然而,NPPV在降低气管插管(NETI)率、死亡率及其他不良事件方面是否优于CPAP仍不明确。我们的目的是回顾这两种方法在ACPE治疗中疗效和安全性的证据。
我们对CPAP和/或NIPV治疗ACPE效果的随机对照试验进行了系统评价和荟萃分析,考虑的结局指标包括NETI、死亡率和急性心肌梗死(AMI)发生率。截至2005年5月,我们检索了6个电子数据库,无语言限制,查阅了相关文章的参考文献,手工检索了会议论文集并联系了专家。
在检索到的790篇文章中,纳入了17篇。汇总分析显示,10项比较CPAP与标准药物治疗(SMT)的研究表明,NETI的绝对风险显著降低22%(95%置信区间(CI),-34%至-10%),死亡率降低13%(95%CI,-22%至-5%)。6项比较NPPV与SMT的研究表明,NETI的绝对风险降低18%(95%CI,-32%至-4%),死亡率降低7%(95%CI,-14%至0%)。7项比较NPPV与CPAP的研究表明,NETI的绝对风险降低3%,无统计学意义(95%CI,-4%至9%),死亡率降低2%(95%CI,-6%至10%)。这些方法均未增加AMI风险。亚组分析显示,在纳入更多高碳酸血症患者的研究中,NPPV的结局并不优于CPAP。
现有充分证据支持在ACPE中使用CPAP和NPPV。与SMT相比,这两种技术均降低了NETI和死亡率,且均未显示增加AMI风险。CPAP应被视为一线干预措施,因为即使在病情更严重的患者中,NPPV也未显示出更好的疗效,且CPAP在临床实践中更便宜且更易于实施。