Mwakyusa Sekela, Wamae Annah, Wasunna Aggrey, Were Fred, Esamai Fabian, Ogutu Bernhards, Muriithi Assumpta, Peshu Norbert, English Mike
KEMRI Centre for Geographic Medicine Research-Coast, P,O, Box 43640, Nairobi, Kenya.
BMC Int Health Hum Rights. 2006 Jul 20;6:9. doi: 10.1186/1472-698X-6-9.
The structured admission form is an apparently simple measure to improve data quality. Poor motivation, lack of supervision, lack of resources and other factors are conceivably major barriers to their successful use in a Kenyan public hospital setting. Here we have examined the feasibility and acceptability of a structured paediatric admission record (PAR) for district hospitals as a means of improving documentation of illness.
The PAR was primarily based on symptoms and signs included in the Integrated Management of Childhood Illness (IMCI) diagnostic algorithms. It was introduced with a three-hour training session, repeated subsequently for those absent, aiming for complete coverage of admitting clinical staff. Data from consecutive records before (n = 163) and from a 60% random sample of dates after intervention (n = 705) were then collected to evaluate record quality. The post-intervention period was further divided into four 2-month blocks by open, feedback meetings for hospital staff on the uptake and completeness of the PAR.
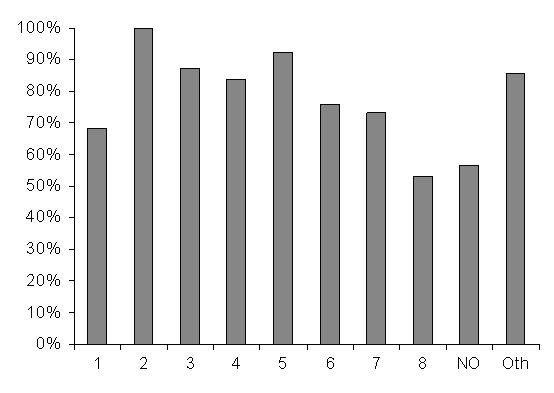
The frequency of use of the PAR increased from 50% in the first 2 months to 84% in the final 2 months, although there was significant variation in use among clinicians. The quality of documentation also improved considerably over time. For example documentation of skin turgor in cases of diarrhoea improved from 2% pre-intervention to 83% in the final 2 months of observation. Even in the area of preventive care documentation of immunization status improved from 1% of children before intervention to 21% in the final 2 months.
The PAR was well accepted by most clinicians and greatly improved documentation of features recommended by IMCI for identifying and classifying severity of common diseases. The PAR could provide a useful platform for implementing standard referral care treatment guidelines.
结构化入院表格看似是一种提高数据质量的简单措施。在肯尼亚公立医院环境中,积极性不高、缺乏监督、资源匮乏以及其他因素可能是其成功使用的主要障碍。在此,我们研究了地区医院结构化儿科入院记录(PAR)作为改善疾病记录方式的可行性和可接受性。
PAR主要基于儿童疾病综合管理(IMCI)诊断算法中包含的症状和体征。通过为期三小时的培训课程引入该记录,随后对缺席者进行重复培训,目标是让所有负责收治的临床工作人员都能接受培训。然后收集干预前连续记录的数据(n = 163)以及干预后60%随机抽取日期的记录数据(n = 705),以评估记录质量。干预后期通过为医院工作人员召开关于PAR使用情况和完整性的公开反馈会议,进一步划分为四个为期两个月的时间段。
PAR的使用频率从最初两个月的50%增加到最后两个月的84%,尽管临床医生之间的使用情况存在显著差异。随着时间的推移,记录质量也有了显著提高。例如,腹泻病例中皮肤弹性的记录从干预前的2%提高到观察期最后两个月的83%。即使在预防保健方面,免疫接种状况的记录也从干预前儿童的1%提高到最后两个月的21%。
PAR得到了大多数临床医生的认可,并极大地改善了IMCI推荐的用于识别和分类常见疾病严重程度的特征记录。PAR可为实施标准转诊护理治疗指南提供一个有用的平台。