Department of Radiation Oncology, University of Wuerzburg, Josef-Schneider-Str, 11, 97080 Wuerzburg, Germany.
Radiat Oncol. 2006 Sep 6;1:34. doi: 10.1186/1748-717X-1-34.
The dose distribution to the rectum, delineated as solid organ, rectal wall and rectal surface, in 3D conformal (3D-CRT) and intensity-modulated radiotherapy treatment (IMRT) planning for localized prostate cancer was evaluated.
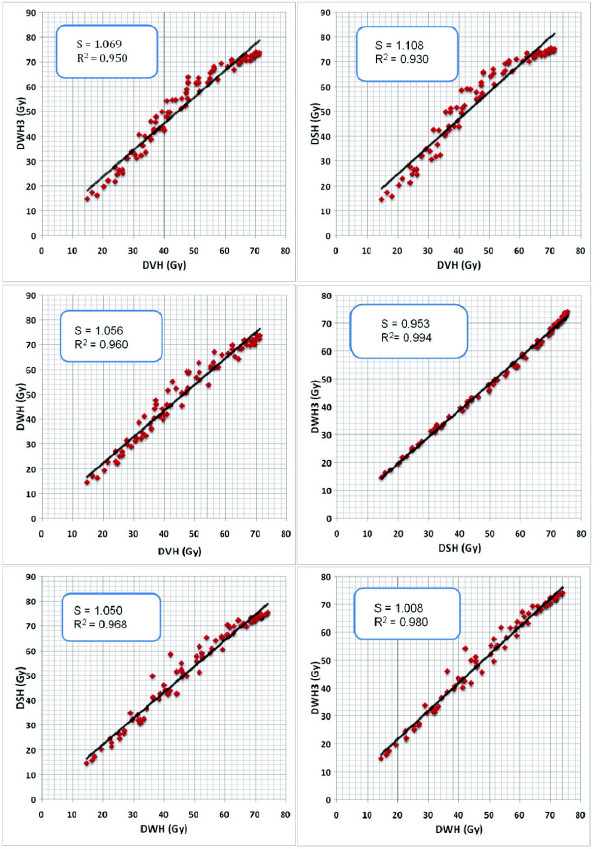
In a retrospective planning study 3-field, 4-field and IMRT treatment plans were analyzed for ten patients with localized prostate cancer. The dose to the rectum was evaluated based on dose-volume histograms of 1) the entire rectal volume (DVH) 2) manually delineated rectal wall (DWH) 3) rectal wall with 3 mm wall thickness (DWH(3)) 4) and the rectal surface (DSH). The influence of the rectal filling and of the seminal vesicles' anatomy on these dose parameters was investigated. A literature review of the dose-volume relationship for late rectal toxicity was conducted.
In 3D-CRT (3-field and 4-field) the dose parameters differed most in the mid-dose region: the DWH showed significantly lower doses to the rectum (8.7% +/- 4.2%) compared to the DWH(3) and the DSH. In IMRT the differences between dose parameters were larger in comparison with 3D-CRT. Differences were statistically significant between DVH and all other dose parameters and between DWH and DSH. Mean doses were increased by 23.6% +/- 8.7% in the DSH compared to the DVH in the mid-dose region. Furthermore, both the rectal filling and the anatomy of the seminal vesicles influenced the relationship between the dose parameters: a significant correlation of the difference between DVH and DWH and the rectal volume was seen in IMRT treatment.
The method of delineating the rectum significantly influenced the dose representation in the dose-volume histogram. This effect was pronounced in IMRT treatment planning compared to 3D-CRT. For integration of dose-volume parameters from the literature into clinical practice these results have to be considered.
在局部前列腺癌的 3D 适形(3D-CRT)和调强放疗(IMRT)计划中,评估了直肠(定义为实体器官)、直肠壁和直肠表面的剂量分布。
在一项回顾性计划研究中,对 10 例局部前列腺癌患者的 3 野、4 野和 IMRT 治疗计划进行了分析。根据 1)整个直肠体积(DVH)2)手动勾画的直肠壁(DWH)3)直肠壁 3mm 壁厚(DWH(3))和 4)直肠表面(DSH)的剂量体积直方图,评估直肠的剂量。研究了直肠充盈和精囊解剖对这些剂量参数的影响。对晚期直肠毒性的剂量-体积关系进行了文献回顾。
在 3D-CRT(3 野和 4 野)中,中剂量区的剂量参数差异最大:DWH 显示直肠(8.7% +/- 4.2%)的剂量明显低于 DWH(3)和 DSH。与 3D-CRT 相比,IMRT 中剂量参数的差异更大。DVH 与所有其他剂量参数之间以及 DWH 与 DSH 之间的差异均具有统计学意义。在中剂量区,DSH 与 DVH 相比,平均剂量增加了 23.6% +/- 8.7%。此外,直肠充盈和精囊解剖均影响剂量参数之间的关系:在 IMRT 治疗中,观察到 DVH 和 DWH 之间的差异与直肠体积之间存在显著相关性。
直肠勾画方法显著影响剂量体积直方图中的剂量表示。与 3D-CRT 相比,这种影响在 IMRT 治疗计划中更为明显。为了将文献中的剂量-体积参数整合到临床实践中,需要考虑这些结果。