Cox Helen, Kebede Yared, Allamuratova Sholpan, Ismailov Gabit, Davletmuratova Zamira, Byrnes Graham, Stone Christine, Niemann Stefan, Rüsch-Gerdes Sabine, Blok Lucie, Doshetov Daribay
The University of Melbourne, Victoria, Australia.
PLoS Med. 2006 Oct;3(10):e384. doi: 10.1371/journal.pmed.0030384.
The DOTS (directly observed treatment short-course) strategy for tuberculosis (TB) control is recommended by the World Health Organization globally. However, there are few studies of long-term TB treatment outcomes from DOTS programs in high-burden settings and particularly settings of high drug resistance. A DOTS program was implemented progressively in Karakalpakstan, Uzbekistan starting in 1998. The total case notification rate in 2003 was 462/100,000, and a drug resistance survey found multidrug-resistant (MDR) Mycobacterium tuberculosis strains among 13% of new and 40% of previously treated patients. A retrospective, observational study was conducted to assess the capacity of standardized short-course chemotherapy to effectively cure patients with TB in this setting.
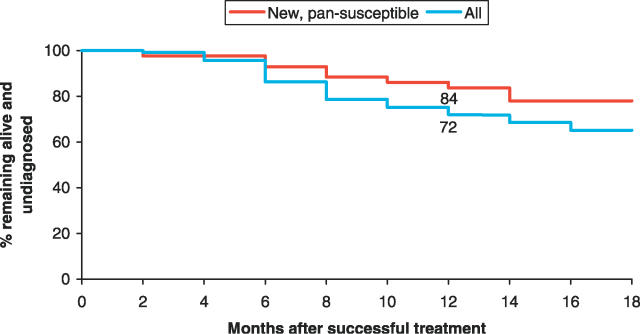
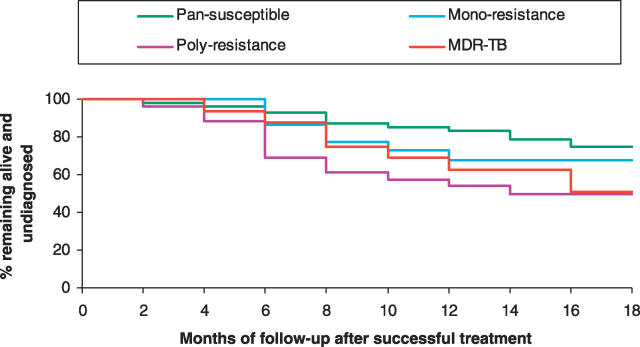
Using routine data sources, 213 patients who were sputum smear-positive for TB, included in the drug resistance survey and diagnosed consecutively in 2001-2002 from four districts, were followed up to a median of 22 months from diagnosis, to determine mortality and subsequent TB rediagnosis. Valid follow-up data were obtained for 197 (92%) of these patients. Mortality was high, with an average of 15% (95% confidence interval, 11% to 19%) dying per year after diagnosis (6% of 73 pansusceptible cases and 43% of 55 MDR TB cases also died per year). While 73 (74%) of the 99 new cases were "successfully" treated, 25 (34%) of these patients were subsequently rediagnosed with recurrent TB (13 were smear-positive on rediagnosis). Recurrence ranged from ten (23%) of 43 new, pansusceptible cases to six (60%) of ten previously treated MDR TB cases. MDR M. tuberculosis infection and previous TB treatment predicted unsuccessful DOTS treatment, while initial drug resistance contributed substantially to both mortality and disease recurrence after successful DOTS treatment.
These results suggest that specific treatment of drug-resistant TB is needed in similar settings of high drug resistance. High disease recurrence after successful treatment, even for drug-susceptible cases, suggests that at least in this setting, end-of-treatment outcomes may not reflect the longer-term status of patients, with consequent negative impacts for patients and for TB control.
世界卫生组织在全球推荐采用结核病直接督导下的短程治疗(DOTS)策略来控制结核病。然而,在高负担地区尤其是高耐药地区,关于DOTS项目长期结核病治疗结果的研究较少。1998年起,乌兹别克斯坦的卡拉卡尔帕克斯坦逐步实施了DOTS项目。2003年的总病例报告率为462/10万,一项耐药性调查发现,13%的新患者和40%的既往治疗患者中存在耐多药结核分枝杆菌菌株。开展了一项回顾性观察研究,以评估标准化短程化疗在此环境下有效治愈结核病患者的能力。
利用常规数据源,对2001年至2002年连续诊断的、来自四个地区且纳入耐药性调查的213例痰涂片阳性结核病患者进行随访,随访时间中位数为自诊断起22个月,以确定死亡率和后续结核病再诊断情况。其中197例(92%)患者获得了有效的随访数据。死亡率很高,诊断后每年平均有15%(95%置信区间为11%至19%)的患者死亡(73例全敏感病例中有6%每年死亡,55例耐多药结核病病例中有43%每年死亡)。虽然99例新病例中有73例(74%)“成功”接受了治疗,但其中25例(34%)患者随后被再次诊断为复发性结核病(13例再诊断时痰涂片阳性)。复发率从43例新的全敏感病例中的10例(23%)到10例既往治疗的耐多药结核病病例中的6例(60%)不等。耐多药结核分枝杆菌感染和既往结核病治疗预示着DOTS治疗不成功,而初始耐药性在DOTS治疗成功后对死亡率和疾病复发均有很大影响。
这些结果表明,在类似的高耐药环境中需要对耐多药结核病进行特异性治疗。即使是对药物敏感病例,成功治疗后疾病复发率也很高,这表明至少在这种环境下,治疗结束时的结果可能无法反映患者的长期状况,从而对患者和结核病控制产生负面影响。