Lee Chih-Hung, Kakinuma Takashi, Wang Julia, Zhang Hong, Palmer Douglas C, Restifo Nicholas P, Hwang Sam T
Dermatology Branch, Center for Cancer Research, National Cancer Institute, Bethesda, Maryland 20892-1908, USA.
Mol Cancer Ther. 2006 Oct;5(10):2592-9. doi: 10.1158/1535-7163.MCT-06-0310.
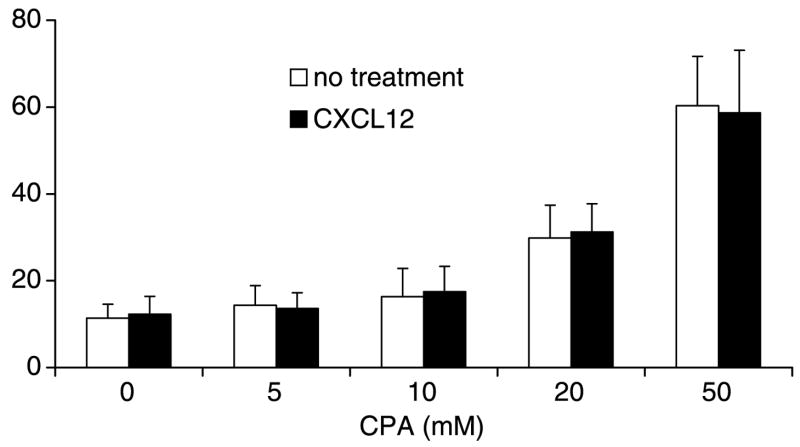
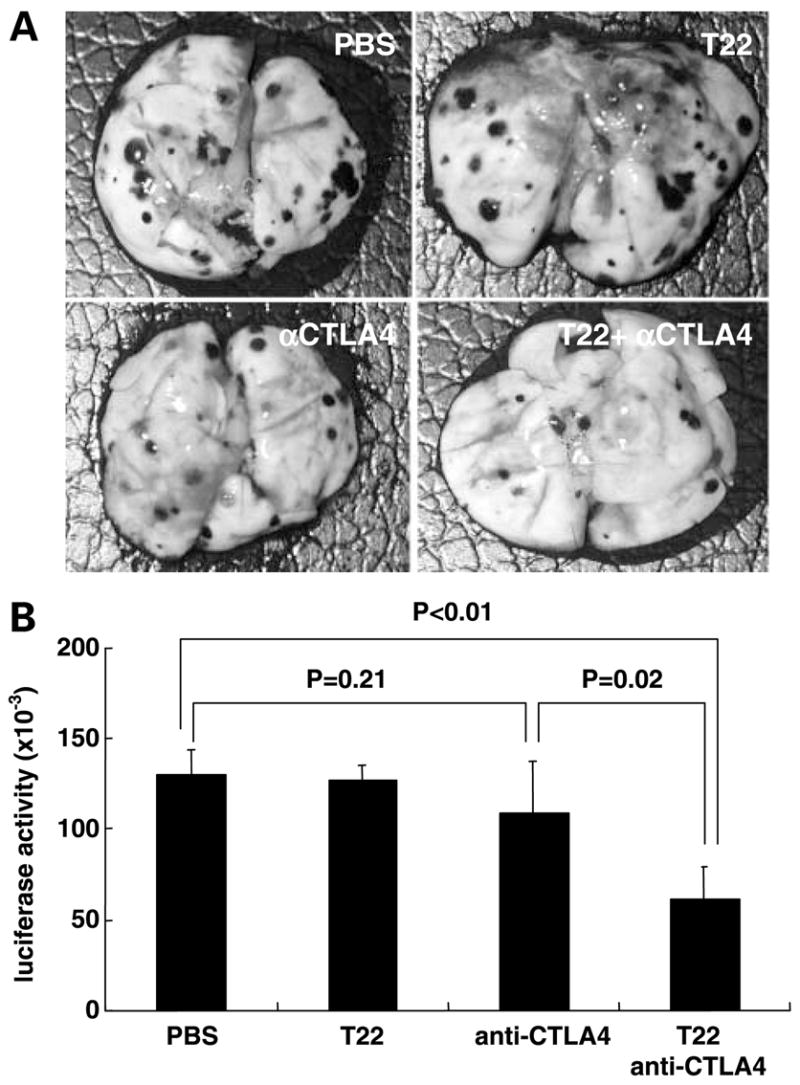
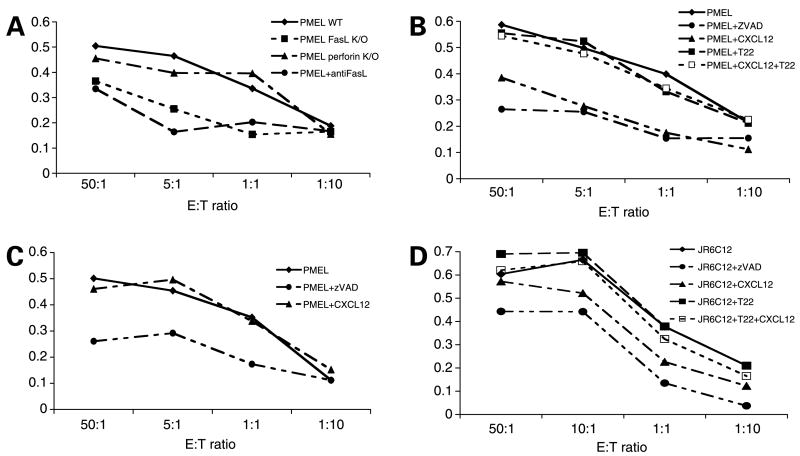
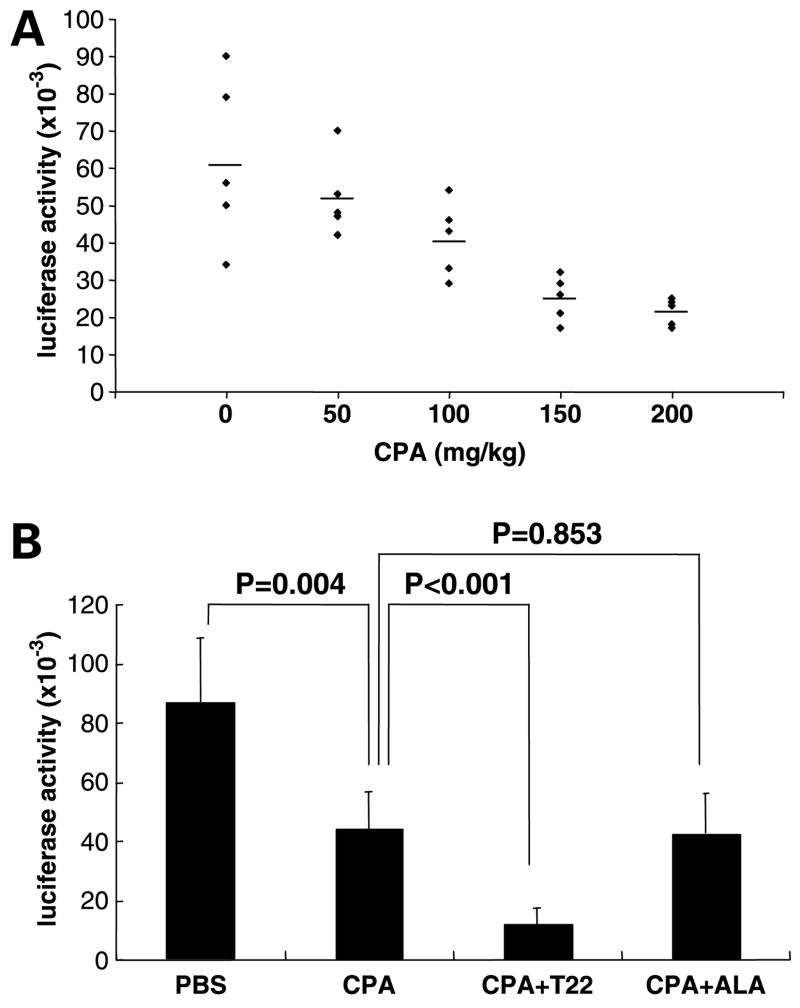
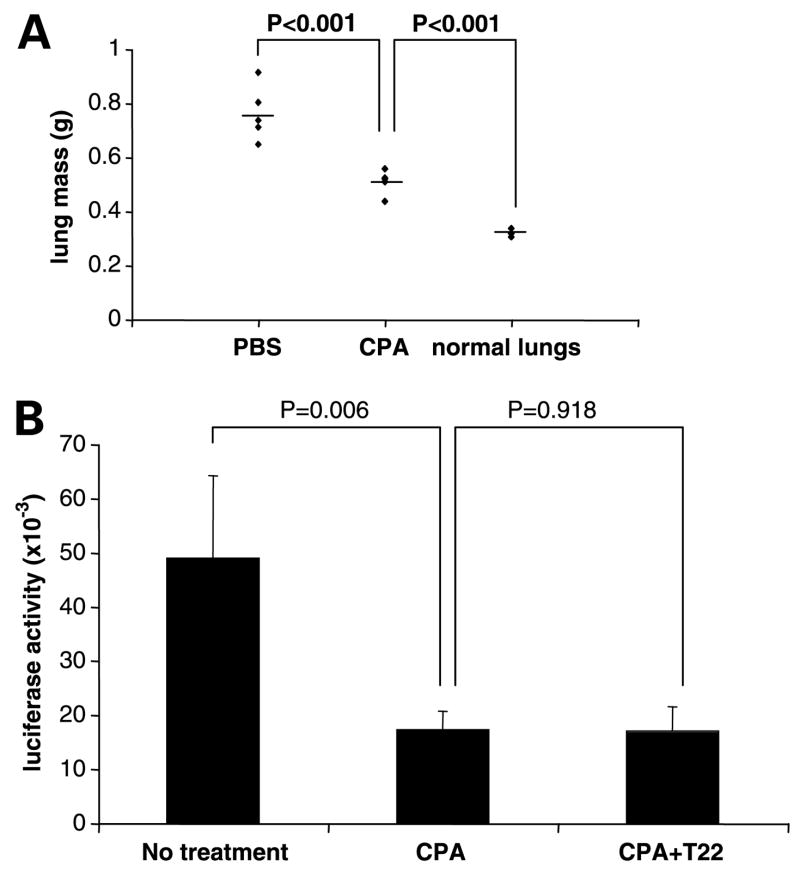
Expression of the chemokine receptor CXCR4 by tumor cells promotes metastasis, possibly by activating prosurvival signals that render cancer cells resistant to immune attack. Inhibition of CXCR4 with a peptide antagonist, T22, blocks metastatic implantation of CXCR4-transduced B16 (CXCR4-luc-B16) melanoma cells in lung, but not the outgrowth of established metastases, raising the question of how T22 can best be used in a clinical setting. Herein, whereas the treatment of CXCR4-luc-B16 cells in vitro with the CXCR4 ligand CXCL12 did not reduce killing induced by cisplatin or cyclophosphamide, CXCL12 markedly reduced Fas-dependent killing by gp100-specific (pmel-1) CD8(+) T cells. T22 pretreatment restored sensitivity of CXCR4-luc-B16 cells to pmel-1 killing, even in the presence of CXCL12. Two immune-augmenting regimens were used in combination with T22 to treat experimental lung metastases. First, low-dose cyclophosphamide treatment (100 mg/kg) on day 5 in combination with T22 (days 4-7) yielded a approximately 70% reduction of B16 metastatic tumor burden in the lungs compared with cyclophosphamide treatment alone (P < 0.001). Furthermore, whereas anti-CTL antigen 4 (CTLA4) monoclonal antibody (mAb; or T22 treatment) alone had little effect on established B16 metastases, pretreatment with T22 (in combination with anti-CTLA4 mAb) resulted in a 50% reduction in lung tumor burden (P = 0.02). Thus, in vitro, CXCR4 antagonism with T22 renders B16 cells susceptible to killing by antigen-specific T cells. In vivo, T22 synergizes with cyclophosphamide or anti-CTLA4 mAb in the treatment of established lung metastases, suggesting a novel strategy for augmenting the efficacy of immunotherapy.
肿瘤细胞表达趋化因子受体CXCR4可促进转移,可能是通过激活促生存信号,使癌细胞对免疫攻击产生抗性。用肽拮抗剂T22抑制CXCR4可阻断CXCR4转导的B16(CXCR4-luc-B16)黑色素瘤细胞在肺部的转移植入,但不能阻止已形成转移灶的生长,这就提出了如何在临床环境中最佳使用T22的问题。在此,虽然用CXCR4配体CXCL12体外处理CXCR4-luc-B16细胞不会降低顺铂或环磷酰胺诱导的杀伤作用,但CXCL12显著降低了gp100特异性(pmel-1)CD8(+) T细胞介导的Fas依赖性杀伤作用。即使存在CXCL12,T22预处理仍可恢复CXCR4-luc-B16细胞对pmel-1杀伤的敏感性。两种免疫增强方案与T22联合用于治疗实验性肺转移。首先,第5天低剂量环磷酰胺治疗(100 mg/kg)与T22(第4 - 7天)联合使用,与单独环磷酰胺治疗相比,肺部B16转移瘤负荷降低了约70%(P < 0.001)。此外,虽然抗细胞毒性T淋巴细胞相关抗原4(CTLA4)单克隆抗体(mAb;或T22治疗)单独对已形成的B16转移灶几乎没有影响,但T22预处理(与抗CTLA4 mAb联合)可使肺部肿瘤负荷降低50%(P = 0.02)。因此,在体外,用T22拮抗CXCR4可使B16细胞易被抗原特异性T细胞杀伤。在体内,T22与环磷酰胺或抗CTLA4 mAb联合治疗已形成的肺转移灶时具有协同作用,提示了一种增强免疫治疗疗效的新策略。