Ghofrani Mohiedean, Tapia Beatriz, Tavassoli Fattaneh A
Department of Pathology, Yale University School of Medicine, Lauder Hall (LH) 222, 310 Cedar St., New Haven, CT 06510, USA.
Virchows Arch. 2006 Dec;449(6):609-16. doi: 10.1007/s00428-006-0245-y. Epub 2006 Oct 13.
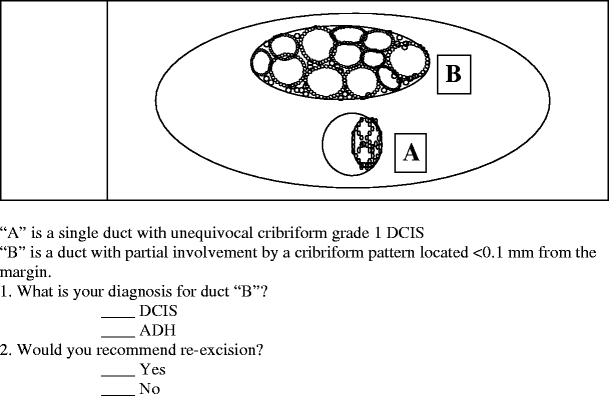
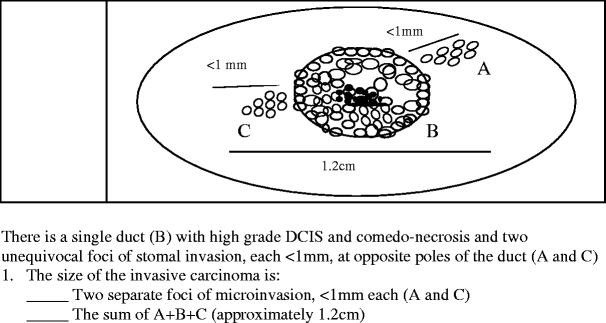
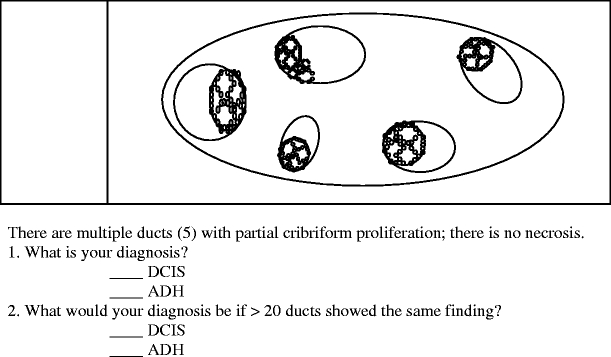
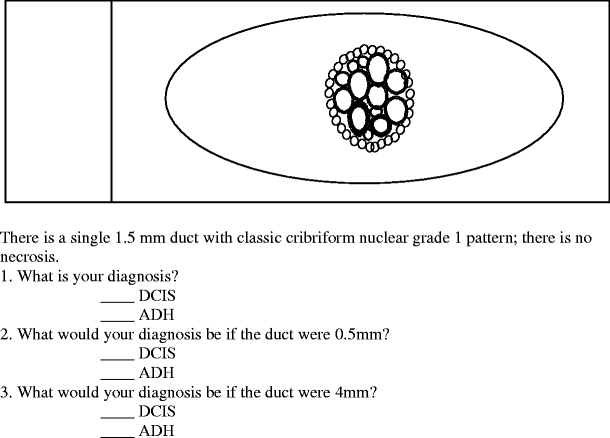
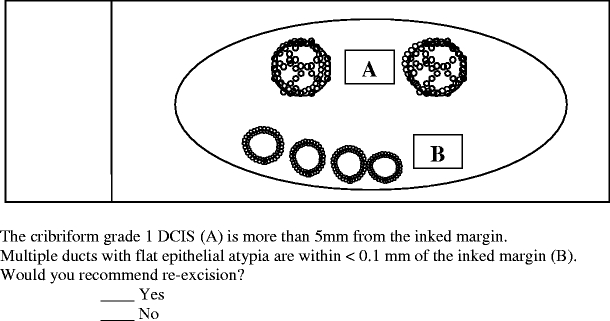
To measure discrepancies in diagnoses and recommendations impacting management of proliferative lesions of the breast, a questionnaire of five problem scenarios was distributed among over 300 practicing pathologists. Of the 230 respondents, 56.5% considered a partial cribriform proliferation within a duct adjacent to unequivocal ductal carcinoma in situ (DCIS) as atypical ductal hyperplasia (ADH), 37.7% of whom recommended reexcision if it were at a resection margin. Of the 43.5% who diagnosed the partially involved duct as DCIS, 28.0% would not recommend reexcision if the lesion were at a margin. When only five ducts had a partial cribriform proliferation, 35.7% considered it as DCIS, while if >or=20 ducts were so involved, this figure rose to 60.4%. When one duct with a complete cribriform pattern measured 0.5, 1.5, or 4 mm, a diagnosis of DCIS was made by 22.6, 31.3, and 94.8%, respectively. When multiple ducts with flat epithelial atypia were at a margin, 20.9% recommended reexcision. Much of these discrepancies arise from the artificial separation of ADH and low-grade DCIS and emphasize the need for combining these two under the umbrella designation of ductal intraepithelial neoplasia grade 1 (DIN 1) to diminish the impact of different terminologies applied to biologically similar lesions.
为了衡量影响乳腺增生性病变管理的诊断和建议差异,向300多名执业病理学家发放了一份包含五个问题场景的问卷。在230名受访者中,56.5%将紧邻明确原位导管癌(DCIS)的导管内部分筛状增生视为非典型导管增生(ADH),其中37.7%的人建议如果其位于切除边缘则进行再次切除。在将部分受累导管诊断为DCIS的43.5%的受访者中,如果病变位于边缘,28.0%的人不建议再次切除。当只有5条导管有部分筛状增生时,35.7%的人将其视为DCIS,而如果有≥20条导管受累,这一比例升至60.4%。当一条具有完整筛状模式的导管测量值为0.5、1.5或4mm时,分别有22.6%、31.3%和94.8%的人做出DCIS的诊断。当多条有扁平上皮异型性的导管位于边缘时,20.9%的人建议再次切除。这些差异大多源于ADH和低级别DCIS的人为划分,并强调需要将这两者合并在导管上皮内瘤变1级(DIN 1)这一统称之下,以减少应用于生物学上相似病变的不同术语的影响。