Njama-Meya Denise, Clark Tamara D, Nzarubara Bridget, Staedke Sarah, Kamya Moses R, Dorsey Grant
Makerere University Medical School, Kampala, Uganda.
Malar J. 2007 Jan 21;6:7. doi: 10.1186/1475-2875-6-7.
Presumptive treatment of malaria in febrile children is widely advocated in Africa. This may occur in the absence of diagnostic testing or even when diagnostic testing is performed but fails to detect malaria parasites. Such over-treatment of malaria has been tolerated in the era of inexpensive and safe monotherapy. However, with the introduction of new artemisinin-based combination therapy (ACT), presumptive treatment becomes economically and clinically less acceptable.
The risks and benefits of only treating children with microscopy confirmed malaria using a prospective cohort design were investigated. A representative sample of 601 children between one and 10 years of age were recruited from a census population in Kampala, Uganda and were followed for all of their health care needs in a study clinic. Standard microscopy was performed each time a child presented with a new episode of fever and antimalarial therapy given only if the blood smear was positive.
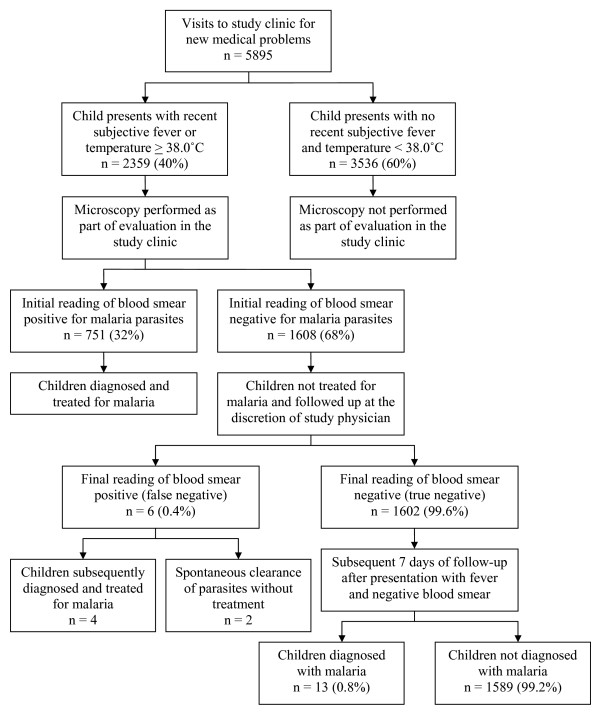
Of 5,895 visits for new medical problems 40% were for febrile illnesses. Of the 2,359 episodes of new febrile illnesses, blood smears were initially reported as negative in 1,608 (68%) and no antimalarial therapy was given. Six of these initially negative smears were reported to be positive following quality control reading of all blood smears: four of these patients were subsequently diagnosed with uncomplicated malaria and two cleared their parasites without antimalarial treatment. Of the 1,602 new febrile illnesses in which the final blood smear reading was classified as negative, only 13 episodes (0.8%) were diagnosed with malaria in the subsequent 7 days. All 13 of these episodes of malaria were uncomplicated and were successfully treated.
In this urban setting, malaria was responsible for only 32% of febrile episodes. Withholding antimalarial therapy in febrile children with negative blood smears was safe and saved over 1,600 antimalarial treatments in 601 children over an 18-month period. In the era of expensive ACT, directing resources towards improving diagnostic and treatment practices may provide a cost-effective measure for promoting rational use of antimalarial therapy.
在非洲,广泛提倡对发热儿童进行疟疾的推定治疗。这种情况可能在未进行诊断检测时发生,甚至在进行了诊断检测但未检测到疟原虫时也会出现。在廉价且安全的单一疗法时代,这种对疟疾的过度治疗一直被容忍。然而,随着新型青蒿素联合疗法(ACT)的引入,推定治疗在经济和临床上变得较难接受。
采用前瞻性队列设计,研究仅对经显微镜确诊疟疾的儿童进行治疗的风险和益处。从乌干达坎帕拉的普查人口中招募了601名1至10岁的儿童作为代表性样本,并在研究诊所满足他们所有的医疗需求。每次儿童出现新的发热发作时都进行标准显微镜检查,只有血涂片呈阳性时才给予抗疟治疗。
在5895次因新的医疗问题就诊中,40%是因发热性疾病就诊。在2359次新的发热性疾病发作中,血涂片最初报告为阴性的有1608次(68%),未给予抗疟治疗。在对所有血涂片进行质量控制复查后,这些最初阴性的血涂片中6次报告为阳性:其中4名患者随后被诊断为非复杂性疟疾,2名患者未接受抗疟治疗寄生虫就清除了。在最终血涂片读数分类为阴性的1602次新的发热性疾病中,在随后7天内只有13次发作(0.8%)被诊断为疟疾。所有这13次疟疾发作均为非复杂性疟疾,且均成功治愈。
在这个城市环境中,疟疾仅占发热发作的32%。对血涂片阴性的发热儿童不给予抗疟治疗是安全的,并且在18个月内为601名儿童节省了超过1600次抗疟治疗。在昂贵的ACT时代,将资源用于改善诊断和治疗方法可能是促进合理使用抗疟治疗的一种具有成本效益的措施。