Solit David B, Ivy S Percy, Kopil Catherine, Sikorski Rachel, Morris Michael J, Slovin Susan F, Kelly W Kevin, DeLaCruz Anthony, Curley Tracy, Heller Glenn, Larson Steven, Schwartz Lawrence, Egorin Merrill J, Rosen Neal, Scher Howard I
Department of Medicine, Memorial Sloan-Kettering Cancer Center, New York, NY 10021, USA.
Clin Cancer Res. 2007 Mar 15;13(6):1775-82. doi: 10.1158/1078-0432.CCR-06-1863.
To define the maximum tolerated dose (MTD), toxicities, and pharmacokinetics of 17-allylamino-17-demethoxygeldanamycin (17-AAG) when administered using continuous and intermittent dosing schedules.
Patients with progressive solid tumor malignancies were treated with 17-AAG using an accelerated titration dose escalation schema. The starting dose and schedule were 5 mg/m(2) daily for 5 days with cycles repeated every 21 days. Dosing modifications based on safety, pharmacodynamic modeling, and clinical outcomes led to the evaluation of the following schedules: daily x 3 repeated every 14 days; twice weekly (days 1, 4, 8, and 11) for 2 weeks every 3 weeks; and twice weekly (days 1 and 4) without interruption. During cycle 1, blood was collected for pharmacokinetic and pharmacodynamic studies.
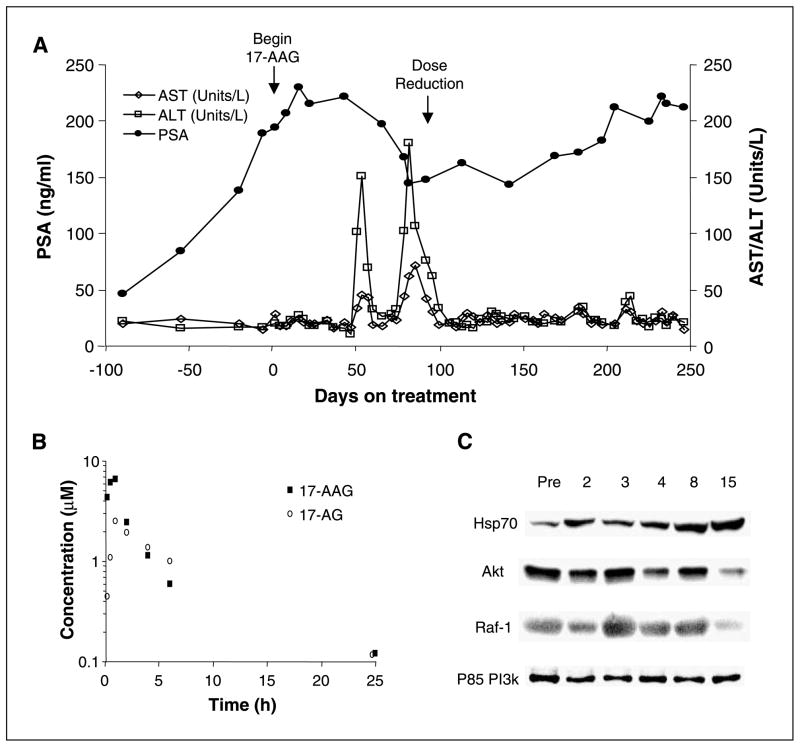
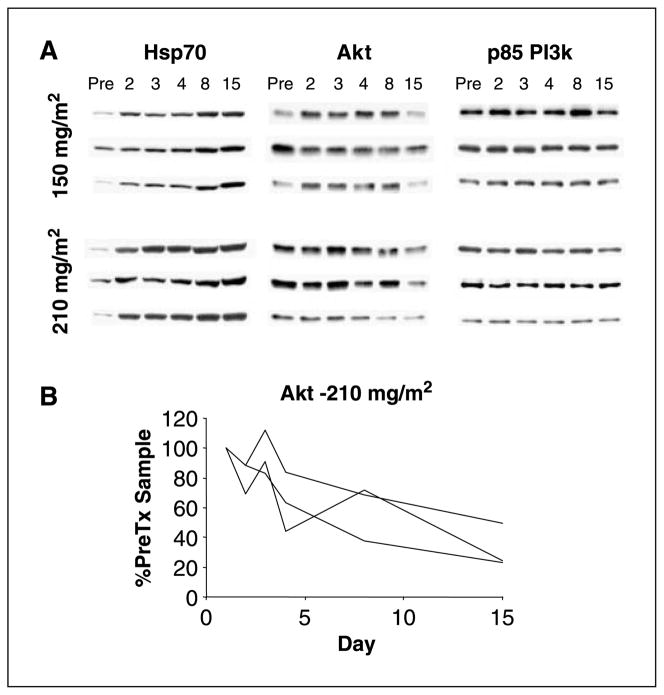
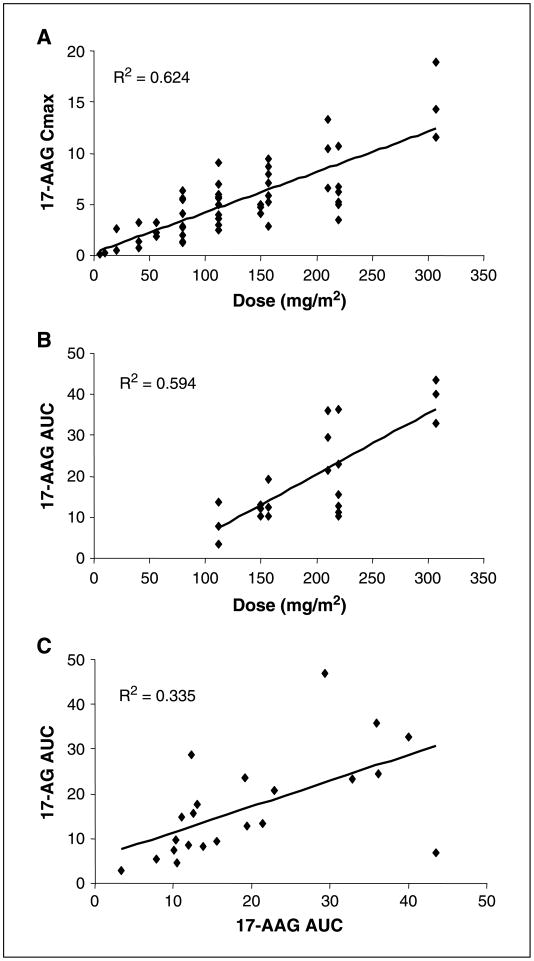
Fifty-four eligible patients were treated. The MTD was schedule dependent: 56 mg/m(2) on the daily x 5 schedule; 112 mg/m(2) on the daily x 3 schedule; and 220 mg/m(2) on the days 1, 4, 8, and 11 every-21-day schedule. Continuous twice-weekly dosing was deemed too toxic because of delayed hepatotoxicity. Hepatic toxicity was also dose limiting with the daily x 5 schedule. Other common toxicities encountered were fatigue, myalgias, and nausea. This latter adverse effect may have been attributable, in part, to the DMSO-based formulation. Concentrations of 17-AAG above those required for activity in preclinical models could be safely achieved in plasma. Induction of a heat shock response and down-regulation of Akt and Raf-1 were observed in biomarker studies.
The MTD and toxicity profile of 17-AAG were schedule dependent. Intermittent dosing schedules were less toxic and are recommended for future phase II studies.
确定采用连续和间歇给药方案给予17-烯丙基氨基-17-去甲氧基格尔德霉素(17-AAG)时的最大耐受剂量(MTD)、毒性及药代动力学情况。
采用加速滴定剂量递增方案,对进展期实体瘤恶性肿瘤患者给予17-AAG治疗。起始剂量和给药方案为每日5mg/m²,共5天,每21天重复1个周期。基于安全性、药效学模型及临床结果进行剂量调整,从而对以下给药方案进行评估:每日给药3次,每14天重复1次;每3周连续2周每周给药2次(第1、4、8和11天);每周给药2次(第1和4天),不间断。在第1周期,采集血液进行药代动力学和药效学研究。
54例符合条件的患者接受了治疗。MTD取决于给药方案:每日给药5次的方案中为56mg/m²;每日给药3次的方案中为112mg/m²;每21天周期中第1、4、8和11天给药的方案中为220mg/m²。连续每周给药2次因肝毒性延迟而被认为毒性过大。每日给药5次的方案中,肝毒性也是剂量限制因素。其他常见毒性包括疲劳、肌痛和恶心。后一种不良反应可能部分归因于基于二甲基亚砜的制剂。血浆中能够安全达到高于临床前模型中活性所需浓度的17-AAG。在生物标志物研究中观察到热休克反应的诱导以及Akt和Raf-1蛋白水平的下调。
17-AAG的MTD和毒性特征取决于给药方案。间歇给药方案毒性较小,推荐用于未来的II期研究。