Fretheim Atle, Håvelsrud Kari, MacLennan Graeme, Kristoffersen Doris Tove, Oxman Andrew D
Norwegian Knowledge Centre for the Health Services, Oslo, Norway.
PLoS Med. 2007 Jul;4(7):e232. doi: 10.1371/journal.pmed.0040232.
The purpose of our study was to evaluate the effects of a new reimbursement rule for antihypertensive medication that made thiazides mandatory first-line drugs for newly treated, uncomplicated hypertension. The objective of the new regulation was to reduce drug expenditures.
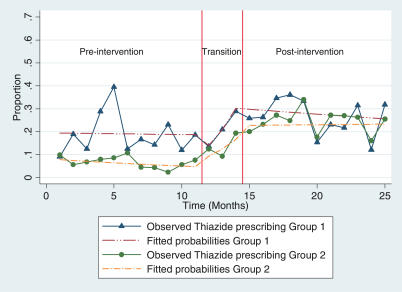
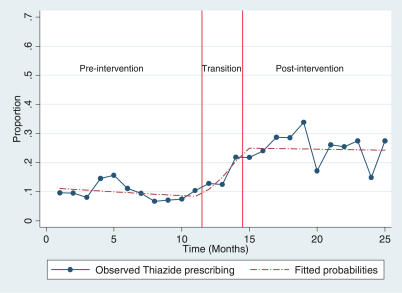
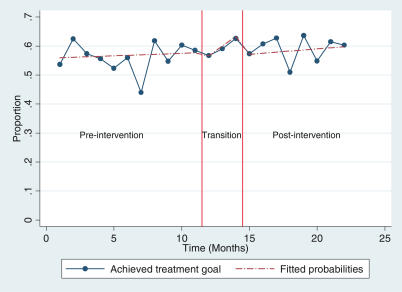
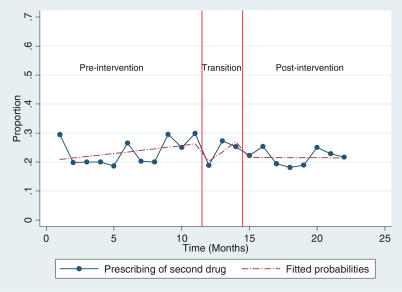
We conducted an interrupted time-series analysis on prescribing data before and after the new reimbursement rule for antihypertensive medication was put into effect. All patients started on antihypertensive medication in 61 general practices in Norway were included in the analysis. The new rule was put forward by the Ministry of Health and was approved by parliament. Adherence to the rule was monitored only minimally, and there were no penalties for non-adherence. Our primary outcome was the proportion of thiazide prescriptions among all prescriptions made for persons started on antihypertensive medication. Secondary outcomes included the proportion of patients who, within 4 mo, reached recommended blood-pressure goals and the proportion of patients who, within 4 mo, were not started on a second antihypertensive drug. We also compared drug costs before and after the intervention. During the baseline period, 10% of patients started on antihypertensive medication were given a thiazide prescription. This proportion rose steadily during the transition period, after which it remained stable at 25%. For other outcomes, no statistically significant differences were demonstrated. Achievement of treatment goals was slightly higher (56.6% versus 58.4%) after the new rule was introduced, and the prescribing of a second drug was slightly lower (24.0% versus 21.8%). Drug costs were reduced by an estimated Norwegian kroner 4.8 million (0.58 million Euros, US$0.72 million) in the first year, which is equivalent to Norwegian kroner 1.06 per inhabitant (0.13 Euros, US$0.16).
Prescribing of thiazides in Norway for uncomplicated hypertension more than doubled after a reimbursement rule requiring the use of thiazides as the first-choice therapy was put into effect. However, the resulting savings on drug expenditures were modest. There were no significant changes in the achievement of treatment goals or in the prescribing of a second antihypertensive drug.
我们研究的目的是评估一项新的抗高血压药物报销规定的效果,该规定将噻嗪类药物定为新治疗的单纯性高血压的一线必备药物。新规定的目标是降低药物支出。
我们对挪威61家普通诊所实施抗高血压药物新报销规定前后的处方数据进行了中断时间序列分析。分析纳入了所有在挪威61家普通诊所开始使用抗高血压药物的患者。新规定由挪威卫生部提出并经议会批准。对规定的遵守情况监测极少,不遵守规定也没有处罚措施。我们的主要结局是开始使用抗高血压药物的患者所开具的所有处方中噻嗪类处方的比例。次要结局包括在4个月内达到推荐血压目标的患者比例以及在4个月内未开始使用第二种抗高血压药物的患者比例。我们还比较了干预前后的药物成本。在基线期,开始使用抗高血压药物的患者中有10%开具了噻嗪类处方。这一比例在过渡期稳步上升,之后稳定在25%。对于其他结局,未显示出统计学上的显著差异。新规定实施后,治疗目标的达成率略高(分别为56.6%和58.4%),第二种药物的处方率略低(分别为24.0%和21.8%)。第一年药物成本估计降低了480万挪威克朗(58万欧元,72万美元),相当于人均1.06挪威克朗(0.13欧元,0.16美元)。
在一项要求将噻嗪类药物作为首选治疗药物的报销规定实施后,挪威用于单纯性高血压的噻嗪类药物处方量增加了一倍多。然而,由此带来的药物支出节省幅度不大。治疗目标的达成情况或第二种抗高血压药物的处方情况没有显著变化。