Tura Olga, Barclay G Robin, Roddie Huw, Davies John, Turner Marc L
SNBTS Adult Cell Therapy Group, Scottish Centre for Regenerative Medicine, University of Edinburgh School of Clinical Sciences, The Chancellor's Building, 49 Little France Crescent, Edinburgh, EH16 4SB, UK.
J Transl Med. 2007 Jul 18;5:37. doi: 10.1186/1479-5876-5-37.
The discovery of adult endothelial progenitor cells (EPC) offers potential for vascular regenerative therapies. The expression of CD34 and VEGFR2 by EPC indicates a close relationship with haematopoietic progenitor cells (HPC), and HPC-rich sources have been used to treat cardiac and limb ischaemias with apparent clinical benefit. However, the laboratory characterisation of the vasculogenic capability of potential or actual therapeutic cell autograft sources is uncertain since the description of EPC remains elusive. Various definitions of EPC based on phenotype and more recently on colony formation (CFU-EPC) have been proposed.
We determined EPC as defined by proposed phenotype definitions (flow cytometry) and by CFU-EPC in HPC-rich sources: bone marrow (BM); cord blood (CB); and G-CSF-mobilised peripheral blood (mPB), and in HPC-poor normal peripheral blood (nPB).
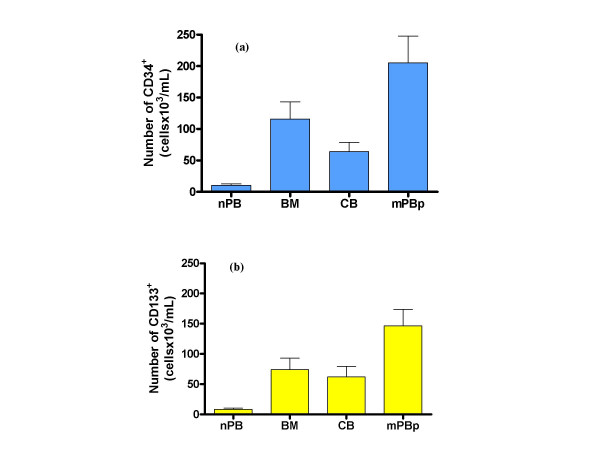
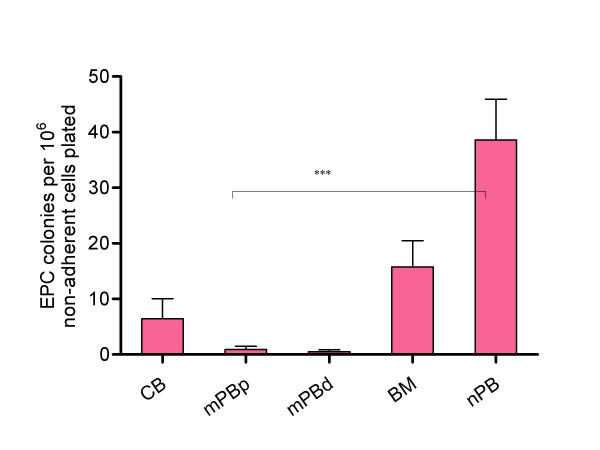
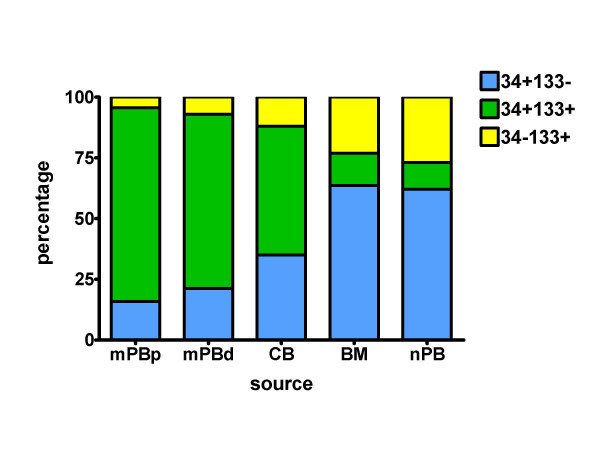
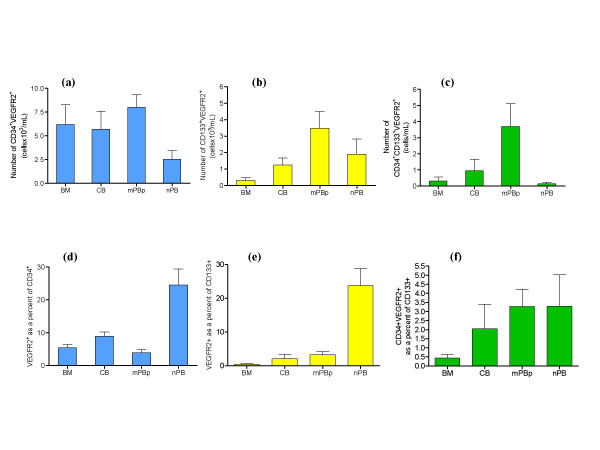
As expected, the highest numbers of cells expressing the HPC markers CD34 or CD133 were found in mPB and least in nPB. The proportions of CD34+ cells co-expressing CD133 is of the order mPB>CB>BM approximately nPB. CD34+ cells co-expressing VEGFR2 were also most frequent in mPB. In contrast, CFU-EPC were virtually absent in mPB and were most readily detected in nPB, the source lowest in HPC.
HPC sources differ in their content of putative EPC. Normal peripheral blood, poor in HPC and in HPC-related phenotypically defined EPC, is the richest source of CFU-EPC, suggesting no direct relationship between the proposed EPC immunophenotypes and CFU-EPC potential. It is not apparent whether either of these EPC measurements, or any, is an appropriate indicator of the therapeutic vasculogenic potential of autologous HSC sources.
成人体内皮祖细胞(EPC)的发现为血管再生治疗带来了希望。EPC表达CD34和VEGFR2表明其与造血祖细胞(HPC)关系密切,富含HPC的来源已被用于治疗心脏和肢体缺血,且具有明显的临床益处。然而,由于EPC的定义仍不明确,潜在或实际治疗性细胞自体移植来源的血管生成能力的实验室特征尚不确定。基于表型以及最近基于集落形成(CFU-EPC)的EPC的各种定义已被提出。
我们根据提出的表型定义(流式细胞术)以及在富含HPC的来源(骨髓(BM)、脐血(CB)和G-CSF动员的外周血(mPB))和HPC含量低的正常外周血(nPB)中的CFU-EPC来确定EPC。
正如预期的那样,表达HPC标志物CD34或CD133的细胞数量在mPB中最多,在nPB中最少。共表达CD133的CD34+细胞比例依次为mPB>CB>BM≈nPB。共表达VEGFR2的CD34+细胞在mPB中也最为常见。相反,CFU-EPC在mPB中几乎不存在,而在HPC含量最低的nPB中最容易检测到。
HPC来源中假定的EPC含量不同。正常外周血中HPC及与HPC相关的表型定义的EPC含量低,但却是CFU-EPC最丰富的来源,这表明所提出的EPC免疫表型与CFU-EPC潜能之间没有直接关系。目前尚不清楚这些EPC测量方法中的任何一种,或是否任何一种,都是自体造血干细胞来源治疗性血管生成潜能的合适指标。