Junius Sara, Haustermans Karin, Bussels Barbara, Oyen Raymond, Vanstraelen Bianca, Depuydt Tom, Verstraete Jan, Joniau Steven, Van Poppel Hendrik
University Hospital Gasthuisberg, Leuven, Belgium.
Radiat Oncol. 2007 Aug 8;2:29. doi: 10.1186/1748-717X-2-29.
To assess acute (primary endpoint) and late toxicity, quality of life (QOL), biochemical or clinical failure (secondary endpoints) of a hypofractionated IMRT schedule for prostate cancer (PC).
38 men with localized PC received 66 Gy (2.64 Gy) to prostate,2 Gy to seminal vesicles (50 Gy total) using IMRT.Acute toxicity was evaluated weekly during radiotherapy (RT), at 1-3 months afterwards using RTOG acute scoring system. Late side effects were scored at 6, 9, 12, 16, 20, 24 and 36 months after RT using RTOG/EORTC criteria.Quality of life was assessed by EORTC-C30 questionnaire and PR25 prostate module. Biochemical failure was defined using ASTRO consensus and nadir+2 definition, clinical failure as local, regional or distant relapse.
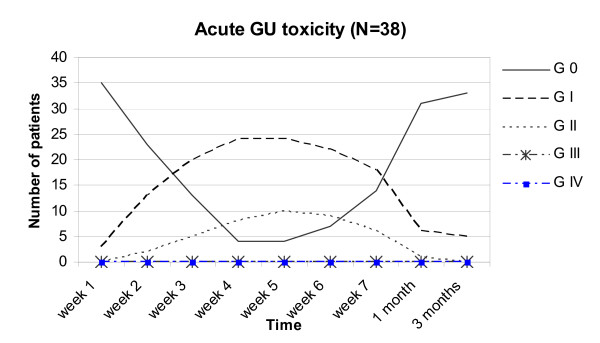
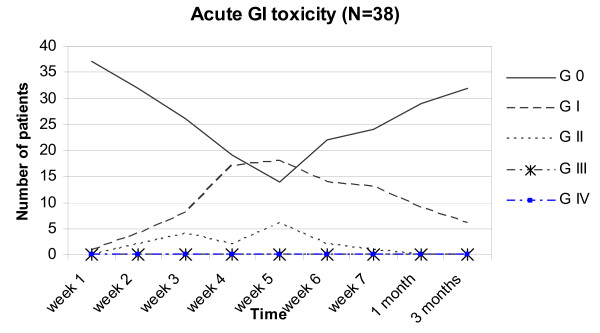
None experienced grade III-IV toxicity. 10% had no acute genito-urinary (GU) toxicity, 63% grade I; 26% grade II. Maximum acute gastrointestinal (GI) scores 0, I, II were 37%, 47% and 16%. Maximal acute toxicity was reached weeks 4-5 and resolved within 4 weeks after RT in 82%.Grade II rectal bleeding needing coagulation had a peak incidence of 18% at 16 months after RT but is 0% at 24-36 months. One developed a urethral stricture at 2 years (grade II late GU toxicity) successfully dilated until now. QOL urinary symptom scores reached a peak incidence 1 month after RT but normalized 6 months later. Bowel symptom scores before, at 1-6 months showed similar values but rose slowly 2-3 years after RT. Nadir of sexual symptom scores was reached 1-6 months after RT but improved 2-3 years later as well as physical, cognitive and role functional scales.Emotional, social functional scales were lowest before RT when diagnosis was given but improved later. Two years after RT global health status normalized.
This hypofractionated IMRT schedule for PC using 25 fractions of 2.64 Gy did not result in severe acute side effects. Until now late urethral, rectal toxicities seemed acceptable as well as failure rates. Detailed analysis of QOL questionnaires resulted in the same conclusion.
评估前列腺癌(PC)的大分割调强放疗(IMRT)方案的急性(主要终点)和晚期毒性、生活质量(QOL)、生化或临床失败(次要终点)。
38例局限性PC男性患者接受IMRT,前列腺照射剂量为66 Gy(2.64 Gy/次),精囊照射剂量为2 Gy(总量50 Gy)。放疗期间每周评估急性毒性,放疗后1 - 3个月使用RTOG急性评分系统评估。放疗后6、9、12、16、20、24和36个月使用RTOG/EORTC标准评估晚期副作用。使用EORTC - C30问卷和PR25前列腺模块评估生活质量。生化失败根据ASTRO共识和最低点+2定义确定,临床失败定义为局部、区域或远处复发。
无患者出现III - IV级毒性。10%的患者无急性泌尿生殖系统(GU)毒性,63%为I级;26%为II级。急性胃肠道(GI)最高评分0、I、II级的患者分别为37%、47%和16%。最大急性毒性在第4 - 5周出现,82%的患者在放疗后4周内缓解。需要凝血的II级直肠出血在放疗后16个月的发生率最高,为18%,但在24 - 36个月时为0%。1例患者在2年时出现尿道狭窄(II级晚期GU毒性),目前已成功扩张。QOL泌尿症状评分在放疗后1个月达到最高发生率,但6个月后恢复正常。放疗前、1 - 6个月时肠道症状评分相似,但在放疗后2 - 3年缓慢上升。性症状评分最低点在放疗后1 - 6个月出现,但在2 - 3年后改善;身体、认知和角色功能量表也有改善。放疗前情绪、社会功能量表最低,但后来有所改善。放疗后2年总体健康状况恢复正常。
这种采用25次分割、每次2.64 Gy的PC大分割IMRT方案未导致严重急性副作用。到目前为止,晚期尿道、直肠毒性以及失败率似乎都是可以接受的。对QOL问卷的详细分析也得出了相同的结论。