Mathews John D, McCaw Christopher T, McVernon Jodie, McBryde Emma S, McCaw James M
Vaccine & Immunisation Research Group, Murdoch Childrens Research Institute and School of Population Health, The University of Melbourne, Parkville, Victoria, Australia.
PLoS One. 2007 Nov 28;2(11):e1220. doi: 10.1371/journal.pone.0001220.
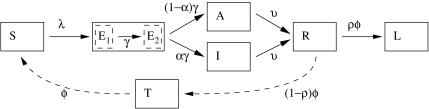
The clinical attack rate of influenza is influenced by prior immunity and mixing patterns in the host population, and also by the proportion of infections that are asymptomatic. This complexity makes it difficult to directly estimate R(0) from the attack rate, contributing to uncertainty in epidemiological models to guide pandemic planning. We have modelled multiple wave outbreaks of influenza from different populations to allow for changing immunity and asymptomatic infection and to make inferences about R(0).
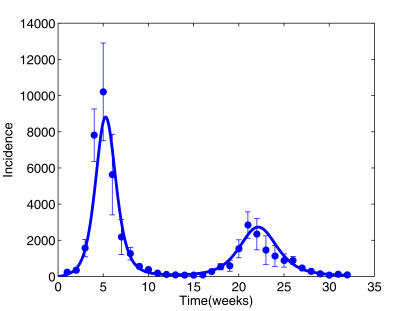
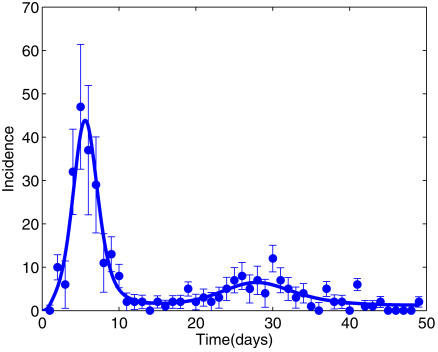
On the island of Tristan da Cunha (TdC), 96% of residents reported illness during an H3N2 outbreak in 1971, compared with only 25% of RAF personnel in military camps during the 1918 H1N1 pandemic. Monte Carlo Markov Chain (MCMC) methods were used to estimate model parameter distributions.
We estimated that most islanders on TdC were non-immune (susceptible) before the first wave, and that almost all exposures of susceptible persons caused symptoms. The median R(0) of 6.4 (95% credibility interval 3.7-10.7) implied that most islanders were exposed twice, although only a minority became ill in the second wave because of temporary protection following the first wave. In contrast, only 51% of RAF personnel were susceptible before the first wave, and only 38% of exposed susceptibles reported symptoms. R(0) in this population was also lower [2.9 (2.3-4.3)], suggesting reduced viral transmission in a partially immune population.
Our model implies that the RAF population was partially protected before the summer pandemic wave of 1918, arguably because of prior exposure to interpandemic influenza. Without such protection, each symptomatic case of influenza would transmit to between 2 and 10 new cases, with incidence initially doubling every 1-2 days. Containment of a novel virus could be more difficult than hitherto supposed.
流感的临床发病率受宿主群体先前免疫力和混合模式影响,也受无症状感染比例的影响。这种复杂性使得难以直接根据发病率估算基本传染数(R₀),导致在指导大流行规划的流行病学模型中存在不确定性。我们对来自不同人群的流感多波暴发进行了建模,以考虑免疫力变化和无症状感染情况,并推断R₀。
在特里斯坦·达库尼亚岛(TdC),1971年H3N2暴发期间96%的居民报告患病,而在1918年H1N1大流行期间,军营里的皇家空军人员只有25%报告患病。采用蒙特卡洛马尔可夫链(MCMC)方法估算模型参数分布。
我们估计,TdC岛上的大多数岛民在第一波疫情之前没有免疫力(易感),并且几乎所有易感人群的接触都导致了症状。中位数R₀为6.4(95%可信区间3.7 - 10.7),这意味着大多数岛民接触了两次,尽管第二波中只有少数人患病,因为第一波后有临时保护。相比之下,第一波疫情之前只有51%的皇家空军人员易感,且只有38%的接触易感者报告有症状。该人群中的R₀也较低[2.9(2.3 - 4.3)],表明在部分免疫人群中病毒传播减少。
我们的模型表明,1918年夏季大流行波之前皇家空军人群受到了部分保护,这可能是因为此前接触过两次大流行之间的流感。如果没有这种保护,每一例有症状的流感病例将传播给2至10例新病例,发病率最初每1至2天翻一番。遏制一种新型病毒可能比迄今认为的更加困难。