Morris-Stiff Gareth, Cheang Peipei, Key Steve, Verghese Anju, Havard Timothy J
Department of Surgery, Royal Glamorgan Hospital, Ynysmaerdy, Llantrisant, UK.
World J Surg Oncol. 2008 Feb 4;6:13. doi: 10.1186/1477-7819-6-13.
Over the course of the past 40 years, there have been a significant number of changes in the way in which lymphomatous disease is diagnosed and managed. With the advent of computed tomography, there is little role for staging laparotomy and the surgeon's role may now more diagnostic than therapeutic.
To review all cases of lymphoma diagnosed at a single institution in order determine the current role of the surgeon in the diagnosis and management of lymphoma.
Computerized pathology records were reviewed for a five-year period 1996 to 2000 to determine all cases of lymph node biopsy (incisional or excisional) in which tissue was obtained as part of a planned procedure. Cases of incidental lymphadenopathy were thus excluded.
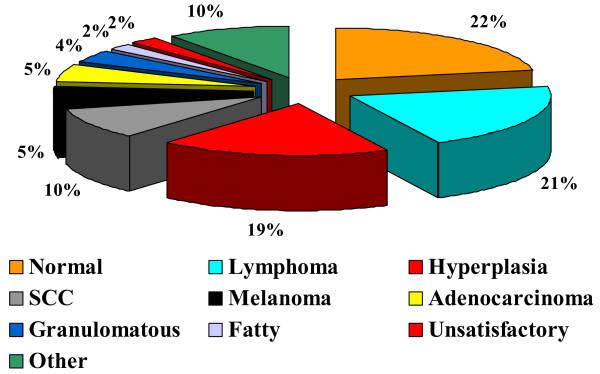
A total of 297 biopsies were performed of which 62 (21%) yielded lymphomas. There were 22 females and 40 males with a median age of 58 years (range: 19-84 years). The lymphomas were classified as 80% non-Hodgkin's lymphoma, 18% Hodgkin's lymphoma and 2% post-transplant lymphoproliferative disorder. Diagnosis was established by general surgeons (n = 48), ENT surgeons (n = 9), radiologists (n = 4) and ophthalmic surgeons (n = 1). The distribution of excised lymph nodes was: cervical (n = 23), inguinal (n = 15), axillary (n = 11), intra-abdominal (n = 6), submandibular (n = 2), supraclavicular (n = 2), periorbital (n = 1), parotid (n = 1) and mediastinal (n = 1). Fine needle aspiration cytology had been performed prior to biopsy in only 32 (52%) cases and had suggested: lymphoma (n = 10), reactive changes (n = 13), normal (n = 5), inadequate (n = 4). The majority (78%) of cervical lymph nodes were subjected to FNAC prior to biopsy whilst this was performed in only 36% of non-cervical lymphadenopathy.
The study has shown that lymphoma is a relatively common cause of surgical lymphadenopathy. Given the limitations of FNAC, all suspicious lymph nodes should be biopsied following FNAC even if the FNAC is reported normal or demonstrating reactive changes only. With the more widespread application of molecular techniques, and the development of improved minimally-invasive procedures, percutaneous and endoscopic techniques may come to dominate, however, at present; the surgeon still has an important role to play in the diagnosis if not treatment of lymphomas.
在过去40年中,淋巴瘤疾病的诊断和治疗方式发生了重大变化。随着计算机断层扫描的出现,分期剖腹术的作用不大,外科医生的作用现在可能更多地是诊断性而非治疗性的。
回顾在单一机构诊断的所有淋巴瘤病例,以确定外科医生目前在淋巴瘤诊断和治疗中的作用。
回顾了1996年至2000年五年期间的计算机化病理记录,以确定所有作为计划程序一部分获取组织的淋巴结活检(切开或切除)病例。因此排除了偶然淋巴结病病例。
共进行了297次活检,其中62例(21%)确诊为淋巴瘤。有22名女性和40名男性,中位年龄为58岁(范围:19 - 84岁)。淋巴瘤分类为80%非霍奇金淋巴瘤、18%霍奇金淋巴瘤和2%移植后淋巴细胞增生性疾病。诊断由普通外科医生(n = 48)、耳鼻喉科医生(n = 9)、放射科医生(n = 4)和眼科医生(n = 1)做出。切除淋巴结的分布为:颈部(n = 23)、腹股沟(n = 15)、腋窝(n = 11)、腹腔内(n = 6)、颌下(n = 2)、锁骨上(n = 2)、眶周(n = 1)、腮腺(n = 1)和纵隔(n = 1)。仅32例(52%)病例在活检前进行了细针穿刺抽吸细胞学检查,提示:淋巴瘤(n = 10)、反应性改变(n = 13)、正常(n = 5)、不充分(n = 4)。大多数(78%)颈部淋巴结在活检前进行了细针穿刺抽吸细胞学检查,而非颈部淋巴结病中仅36%进行了此项检查。
该研究表明淋巴瘤是外科淋巴结病的一个相对常见原因。鉴于细针穿刺抽吸细胞学检查的局限性,即使细针穿刺抽吸细胞学检查报告正常或仅显示反应性改变,所有可疑淋巴结在细针穿刺抽吸细胞学检查后均应进行活检。随着分子技术的更广泛应用以及改进的微创手术的发展,经皮和内镜技术可能会占据主导地位,然而,目前;外科医生在淋巴瘤的诊断(即使不是治疗)中仍可发挥重要作用。