Bisson Gregory P, Gaolathe Tendani, Gross Robert, Rollins Caitlin, Bellamy Scarlett, Mogorosi Mpho, Avalos Ava, Friedman Harvey, Dickinson Diana, Frank Ian, Ndwapi Ndwapi
University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania, USA.
PLoS One. 2008 Mar 5;3(3):e1725. doi: 10.1371/journal.pone.0001725.
Monitoring the effectiveness of global antiretroviral therapy scale-up efforts in resource-limited settings is a global health priority, but is complicated by high rates of losses to follow-up after treatment initiation. Determining definitive outcomes of these lost patients, and the effects of losses to follow-up on estimates of survival and risk factors for death after HAART, are key to monitoring the effectiveness of global HAART scale-up efforts.
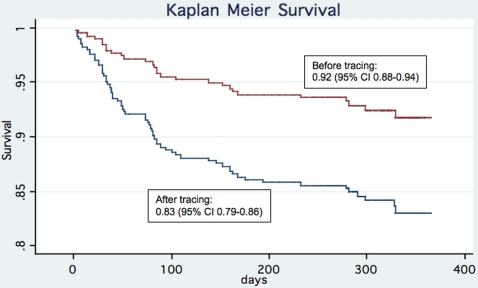
METHODOLOGY/PRINCIPAL FINDINGS: A cohort study comparing clinical outcomes and risk factors for death after HAART initiation as reported before and after tracing of patients lost to follow-up was conducted in Botswana's National Antiretroviral Therapy Program. 410 HIV-infected adults consecutively presenting for HAART were evaluated. The main outcome measures were death or loss to follow-up within the first year after HAART initiation. Of 68 patients initially categorized as lost, over half (58.8%) were confirmed dead after tracing. Patient tracing resulted in reporting of significantly lower survival rates when death was used as the outcome and losses to follow-up were censored [1-year Kaplan Meier survival estimate 0.92 (95% confidence interval, 0.88-0.94 before tracing and 0.83 (95% confidence interval, 0.79-0.86) after tracing, log rank P<0.001]. In addition, a significantly increased risk of death after HAART among men [adjusted hazard ratio 1.74 (95% confidence interval, 1.05-2.87)] would have been missed had patients not been traced [adjusted hazard ratio 1.41 (95% confidence interval, 0.65-3.05)].
CONCLUSIONS/SIGNIFICANCE: Due to high rates of death among patients lost to follow-up after HAART, survival rates may be inaccurate and important risk factors for death may be missed if patients are not actively traced. Patient tracing and uniform reporting of outcomes after HAART are needed to enable accurate monitoring of global HAART scale-up efforts.
在资源有限的环境中监测全球抗逆转录病毒治疗推广工作的有效性是一项全球卫生重点,但治疗开始后随访失访率很高,这使监测工作变得复杂。确定这些失访患者的确切结局以及随访失访对高效抗逆转录病毒治疗(HAART)后生存率估计和死亡风险因素的影响,是监测全球HAART推广工作有效性的关键。
方法/主要发现:在博茨瓦纳国家抗逆转录病毒治疗项目中开展了一项队列研究,比较了随访失访患者追踪前后报告的HAART开始后临床结局和死亡风险因素。对410名连续接受HAART的HIV感染成人进行了评估。主要结局指标为HAART开始后第一年内死亡或失访。在最初归类为失访的68名患者中,超过一半(58.8%)在追踪后被证实死亡。当以死亡为结局且对随访失访进行审查时,患者追踪导致报告的生存率显著降低[1年Kaplan Meier生存率估计值:追踪前为0.92(95%置信区间,0.88 - 0.94),追踪后为0.83(95%置信区间,0.79 - 0.86),对数秩检验P<0.001]。此外,如果未对患者进行追踪,将会遗漏男性HAART后死亡风险显著增加这一情况[调整后风险比1.74(95%置信区间,1.05 - 2.87)] [调整后风险比1.41(95%置信区间,0.65 - 3.05)]。
结论/意义:由于HAART后随访失访患者的死亡率很高,如果不积极追踪患者,生存率可能不准确,并且可能遗漏重要的死亡风险因素。需要对患者进行追踪并统一报告HAART后的结局,以便准确监测全球HAART推广工作。